Thanks PP - don’t worry about the rushed format, I’m going to be worse!
I accept what you are saying about undercounting in the developing world. I expect these countries are being deprived of vaccines anyway - until they can jolly well stump up for them full whack - so probably doesn’t change the essence!?
PP: “myocarditis: I remember reading that a young person was 6x more likely to get myocarditis from covid than the vaccine. Ill have to look that up again. Also I remember that we are inly talking about somethibg likr 3/4 cases per 100,000 in the highest risk groups (It’s been a while since ive looked at those numbers) - hence small effect”
That may be an old figure, when myocarditis was in denial. In any case it’s misleading because it applies to people who actually have covid.
There’s a study that told us, I’m sure there have been others.
5/7/22 A study reported in JAMA Cardiology on April 20 carries the eye-popping title of: “SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents.”
" Specifically, among young men receiving two doses of the same vaccine, between four and seven excess myocarditis and pericarditis events occurred in 28 days per 100,000 vaccinees after the second dose of the Pfizer vaccine, and between nine and 28 excess myocarditis and pericarditis events occurred per 100,000 vaccinees after the second dose of the Moderna vaccine."
Risk increases with dose. Important.
Study here, SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents - PubMed
Yes I acknowledged you were replying to a claim about more people dying from the vaccine than covid. But we are allowed to use our brains (for the time being  ). So I would like to know what you make of this comparison.
). So I would like to know what you make of this comparison.
“Are there huge spikes? Above the normal background level?”
Well probably, if you allow for the underreporting. The sampling estimate was 10-100 times. I was avoiding ‘normal background level’ (because due to VAERS underreporting, that’s a bias that I’m sure you would MUCH rather commit to enthusiastically embracing the next prime minister, than knowingly benefit from in your argument  ) but I’ll look at that in a minute.
) but I’ll look at that in a minute.
The HUGE (how do you get a bigger font dammit ) spike I mentioned actually referred to the jump in the adverse event reports for vaccines. I simply compared the AERs of Covid-19 vaccines to AERs of other vaccines in the same year (2021). The other vaccines combined, on a very quick look, compare in numbers to the covid jabs, if they don’t actually outnumber them. Without knowing actual vaccine totals, it can only be a rough comparison but isn’t unfair to the covid jabs.
So again:
“But on Vaers, what analysis do you need when a new vaccine appears and there are immediately HUGE spikes in several serious adverse events (myocarditis, pulmonary embolisms, pericarditis), all more serious than Covid. These were spikes of 100,1000 times the previous rates associated with vaccines. And they persisted all year so weren’t down to topicality. The spike in vaccine deaths are similar”
Myocarditis reported in VAERS was 80 times higher for covid vaccines than all other vaccine combined, and as I say I think that’s a comparable number of jabs. For Pulmonary embolisms it was 200 times higher. There’s a host of these comparisons.
Even if we don’t have the comparison against ‘background rates’ - these can vary quite a bit depending on the locations, and when the figures were gathered - would you accept this requires explanation?
But on comparison vs background rates, I do have some thumbnail figures, offered with caveat:
" Dilated cardiomyopathy (DCM) is the most common form of cardiomyopathy and cause of cardiac transplantation in children.
…The annual incidence of DCM in children younger than 18 years was 0.57 cases per 100,000 per year overall. The annual incidence was higher in boys than in girls (0.66 vs 0.47 cases per 100,000; P<.001), in blacks than in whites (0.98 vs 0.46 cases per 100,000; P<.001), and in infants (<1 year) than in children (4.40 vs 0.34 cases per 100,000; P<.001)" (2006, US+C, Incidence, causes, and outcomes of dilated cardiomyopathy in children - PubMed)
“0.9 per 100,000 children in 2016”, US again Trends in Acute Myocarditis Related Pediatric Hospitalizations in the United States, 2007-2016 - PubMed
“an annual incidence of 1.24 per 100,000 children younger than 10 years of age”, (Australia 2003) The epidemiology of childhood cardiomyopathy in Australia - PubMed
So that annual incidence of myocarditis for the U18 population - between 0.6 and 1.2 per 100,000?
Call it 0.9 per 100,000.
How many jabbed are there in the under 18 range? A guess: 335m US population, maybe 85m under-18? I’m looking only at 2021 for the Vaers data.
Without looking them up maybe half of the older kids were vaxed in 2021? Half of the older half…maybe 21 million? (My statistical robustness is going out the window here )
That’s our 2021 US jabbed population, according to …me. 21 million kids.
…according to the to the estimates, 0.9 per 100,000 of whom would normally get myocarditis in a year. ie about 0.9 x 21 times a million divided by 100,000 = about 189.
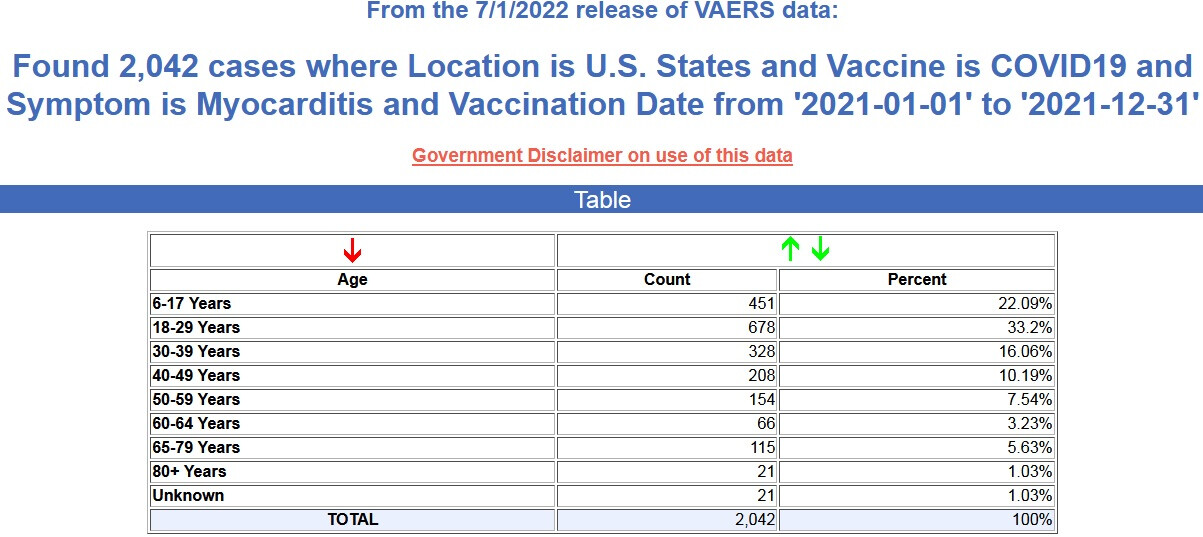
This is to be compared to the Vaers. Vaers gives us this table:
According to the Table there were 451 Myocarditis reports from the covid-19 jabs in 2021.
That’s more than double my estimate of 189. Now that 189 could be an undercount, probably is maybe a factor of two.
But it doesn’t take into account the much greater underreporting in Vaers.
Cheers