Bloody hell, Pat, this this is awful stuff! A libertarian stiff with far too much money walks through a disgustingly over-prosperous neighbourhood where he has a house - with NO pedestrian pavements, note - neglecting both the traffic-safety of his dog, and also where she shits on his neighbours’ property - whilst he masturbates his crack-brained prejudices (making just occasional sense), and includes a brief clip of Mullis talking about PCR. We should listen to this stuff because he makes occasional sense about covid, Fauci and PCR?
I hope he ends up homeless and destitute. Then we’ll see how laid-back cool he is about losing so much (hallucinatory, anyway) money! Once he displayed the usual USAmerican ignorance about the actual meaning of the word ‘communism’ - and of course about Cuba and Venezuela - I’d had about enough.
There are plenty of people who are calling out the scamdemic for what it is, and nailing people like Fauci and ilk for the Nurnberg criminals that they are, without feeling the need to pile on their prejudices about other irrelevant stuff.
Weird glitch: I notice that I’m added as a poster who likes this post. Don’t know how it got there, and it certainly isn’t true, but I can’t see how to delete it.
Sorry, Pat! No offence intended to you. I just had some serious confusion creeping in, listening to this man’s weird collection of half-baked ideas, right alongside his scattering of accurate ones. Should follow his own advice and - as he asserts Gates needs to do - do something about his own skinny muscles and fat flab-belly.
Once again: Sorry Pat! No offence intended. Peace!
Didn’t stick around for long after the relevant couple of minutes but a good summery.
The speed at which the narrator babbles took some following, rather like one of those sales people desperate to list all the great reasons why you need this thing you’d never heard of a minute ago.
Hi Pat, thanks for your response. Can I just say where I agree and where I disagree?
Yes, far too much was made of the PCR test. It’s not a bad test it’s just only half the picture. Most of the criticisms have some validity, I think the problem is the leap to ‘nothingness’. This leap is easily shot down by existing information, leaving the public to be misled by a (scientifically) bland and superficial (misleading) narrative while a strong case against the policy isn’t being heard. Not least, the need to treat people who do get covid early hardly gets a mention except for the purpose of suppressing it.
I agree with the criticism of ‘cases’, but that doesn’t mean the PCR test has no meaning (I’ll indicate something definitely useful further down).
As you’ll know the way it’s supposed to work (a la Mullins?) is that if you have covid symptoms, and a PCR test is positive, there is a ‘likelihood’ that you have covid-19.
I say ‘likelihood’ because there is an overlap in the list of symptoms with those of flu. So if you happen to have some sars-cov2 fragments lying around when you catch the flu, it’s likely you will become a diagnosed covid-19 ‘case’ instead due to the testing policy, and of course the lack of flu tests.
I agree there is no usefulness when there is no corroboration - ie there are no symptoms, or other strong suspicion that somebody has covid-19 like someone found to have had symptoms in an event where exposure was likely.
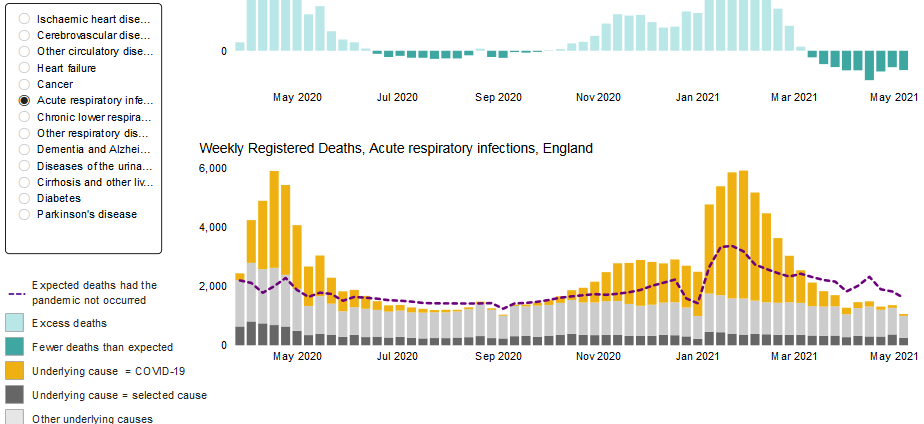
You can see the PCR-useful and PCR-nonuseful periods in the data (graph at the bottom) but let me explain what to look out for, as despite appearances, the two ‘waves’ are different and actually show the differing effect of PCR.
In the first wave, nobody had prior exposure to sars-cov2, and also they only tested people with symptoms - so anybody testing positive at least had viable virus. So, in April-May last year the excess deaths and the ‘covid deaths’ coincided (though there would be some deaths where covid played no role but let’s set that aside for now). Knowing that most of the excess deaths related to covid-19 was useful in theory - or should have been.
But in the second wave many people would have already had the virus or exposure to it, and would have these fragments. And by then there was testing like mad so these would be picked up and called covid cases. That’s where the PCR was now very misleading in finding and counting those fragments and then calling them cases and even ‘infections’.
And this blatant error shows clearly in the excess deaths in the second wave - because the ‘covid deaths’ in that period significantly exceed the excess deaths, meaning there was some over-counting. This over-counting represents nonviable viral fragments in people with no symptoms.
There’s a graph here with the excess deaths and covid deaths
If you can bear with me…you have to make some sort of choice.
The graphs show excess deaths and the ‘covid-19 deaths’ for every week since the beginning.
These are shown in separate graphs but we want to see them on the same graph with the usual dotted line indicating five-year average deaths. As it happens this is only shown when the graph is subdivided by ‘cause of death’ but it’s the same for almost every cause.
So if you select ‘cause of death’ (only to see graphs with the dotted line) and choose almost any of the illnesses…say acute respiratory.
The key is the dotted line - the five-year average deaths for that week. The yellow shows the part that is ‘covid deaths’.
What stands out in the SECOND wave for almost all of the causes of death shown is that if you removed the covid (say you disappeared the yellow) the deaths would fall way below the five year average. This indicates that they are not REALLY covid deaths - because if there was no covid, a significant number of expected deaths would not appear.
This is not so in the FIRST wave - all the yellow is above the dotted line - i.e. the covid deaths were, at least, all ‘excess’ to normal deaths.
And the fact this feature isn’t present in the first wave indicates it’s due to the PCR test on which covid deaths were based having a different effect.
I agree PCR is misused. A positive PCR test means you’re ‘more likely’ to have viable sars-cov2 virus than if you have a negative test. That has been exploited - on its own it doesn’t mean much but of course the ‘health’ system then makes its own leap - you have THE VIRUS! Forget the second part, symptoms or corroborating factors.
" But in my book, if it was really a novel Corona virus, there would be no need to hijack the worlds media, censor every dissenting voice, and offer burgers, fries, ice creams and lottery tickets for people to take the jab."
Well yes - there is a political drive to exaggerate everything and mislead people so that they follow the narrative. But that doesn’t mean it’s based on nothing, or that there is no virus in the first place. Some of us want to tell the government (and the public) that the govt should be curing the virus early on - that others are saying doesn’t really exist!
I couldn’t find the Mullins video but I agree with what you say there - cases aren’t necessarily sick people - and what is a good test is being misused by making it the whole picture.
Excellent analysis and logic ED - and my position pretty accurately - as well as my agreement that the total COVID denial makes things worse for the true science. A similar case is of last night’s SBS prog on vaccine hesitancy, where the guy visited a known COVID resistance hotspot in N NSW and spoke to a group of people. They all had comments to make that were sensible with a range of points, but every one was cut off except the guy who said “they want to implant a chip in every living human being”. This little clip was also used to advertise the programme. We are really getting the big VAX push here at the moment, with a new outbreak threatening that has suddenly made people drop their hesitancy. VAX clinics were sitting idle till yesterday, and now they are packed out. Meanwhile a testing lab made 12% on it daily share price today…
What I wanted to say in reply to Pat B was about a specific piece of research which I came upon through Didier Raoult - on a specific patient who survived for 152 days with CV infection, four courses of Remdesevir, and the evolution of several new strains of virus in his body. Raoult said this man was the original source of the UK Strain outbreak in Kent, coming across from Belgium I think. And who am I to question him!
The first page of this paper describes what happened with this extraordinarily sick man, but with a special emphasis here on the number of cycles to get a positive test. His CT varied from over 36 - when he was said to be free of the virus, down to 20 and then 15 before he finally succumbed. Raoult considers the defining point to be 32 cycles, above which “cases” are unlikely to be infective or have symptoms, so are irrelevant.
There is an appendix to this paper of some 40 pages, with illustrations and graphs, which are very interesting if you have a head for detail. And it’s frankly impossible to say that the virus “doesn’t exist” in the face of this. And as noted above, if the virus doesn’t exist then all talk about the way young people are immune and herd immunity is now prevalent in the UK is irrelevant.
While it is possible that many people without sufficient science background have come on these extreme covid-denial ideas, sometimes I think perhaps they are planted there by the Hasbara collective, or seeded into appropriate communities the way that fear has been seeded into them. Being able to dismiss every alternative as mad conspiracy theory is VERY convenient for the malignant powers that be.
Thanks Karen, interesting, and need to keep an eye on this lot, as well as Globsec and First Draft, who seem to be coordinating the disinformation ecosphere.
William Tucker links to this report from the UN about deaths of children and mothers resulting from deprivation of ordinary services - sucked dry by COVIDAID. The article also details other tragedies - 400, million children missing school, 3.2 million more unplanned pregnancies.
Yes, there’s a nasty new flu about, a bit worse than the average, though not much. It kills some people, as flus always do, every year. But no, there’s no global pandemic health emergency. That’s just gangsters-on-the-make and their tabaquis pushing a vast scam.
There is in fact a choice of effective treatments for covid-flu already freely available in plenty, proven by frontline doctors over the past fifteen months, which stop the illness in days, with next to no lives lost, apart from the odd patient who’s already very ill with other problems. These treatments are all cheap, safe, well proven and tested, officially approved for use, and mostly out of patent.
In any case, the recovery rate from covid for all categories is over 95 percent. For anyone in passably good health below 70 it’s over 99.9 percent. The all-causes death toll during the covid scam is comparable with recent averages, with NO enormous uptick: the basic definition of a real pandemic. There is NO global health emergency.
None of the destructive rules put in place to ‘fight covid’ are effective. All of them are deleterious in their own right. This flu is now largely endemic, with most exposed populations already well into herd immunity. Their immune systems now mostly have a fully-balanced, long-term defence against this flu, as also against previous strains.
Speaking of strains and ‘variants’: pathogens do this variation all the time. In the case of covid, none of them matter a damn, and none are worth worrying about, since ALL of them are so closely similar to the original as to be easily identified and neutralised by the immune response. BTW, someone somewhere MAY have a fully-purified sample of the alleged SARS-COV2 pathogen, but if so, they’re keeping a low profile. No search for authentic, fully-proven samples has turned up anything convincing, so far, in the public domain. The alleged profiles are mostly from computer modelling - where GIGO rules - together with simple guesswork by the computer-virologist sect.
The poison-stabs are a huge con, and a huge crime against humanity, for which the perpetrators have to be hauled before a Nurnberg 2 tribunal. The stabs, in three words, are: Unnecessary, Ineffectual, and Dangerous - but enormously profitable for the criminal gangsters pushing them.
Kary Mullis’s PCR process is a wonderful creation - for its proper purpose. But as Mullis pointed out repeatedly, it’s not a test, for covid-flu or anything else. All conclusions drawn from its use as a ‘test’ are fake, and are to be discounted root and branch. We have no fully clear picture of the true status of this pathogen at present, because the powers-that-shouldn’t-be are refusing to do - or to allow through the censorship system - any actually sound science to get one. Instead, they continue to push the con, some out of mistaken good faith, many of the more invertebrate simply out of cravenly going along to get along, and some out of sheer criminal purpose.
This seems to me to be the true picture of the scam, as it’s now coming clear. And although many will be so horrified and shocked by the idea of a huge bad-faith con being perpetrated by people we’re supposed to trust, that they have deep emotional difficulty in taking it on board, nevertheless, none of the above is loony cospithirry, and all of it can be backed by masses of persuasive real evidence; which continues to pile up.
This account is accurate enough to convince anyone who’s actually willing and able to survey the information on which it rests. It doesn’t lend itself to propagandists ridiculing it as loony nonsense. Savvy people of any kind can see this and take it soberly, if they choose.
1. IN 1993, the biochemist Dr Kary Mullis won the Nobel prize for inventing the PCR (polymerase chain reaction) technique.
It was designed to analyse DNA in a cost-effective and expedient way by replicating a strand of DNA millions of times, allowing scientists to pinpoint a segment of the strand and amplify it. Polymerase is an enzyme which is essential for producing DNA and RNA.
Mullis’s revolutionary method was used to detect genetic mutations to identify genetic diseases such as sickle cell anaemia. It was never designed to diagnose infectious diseases .
2. In a 1993 interview, Mullis candidly spoke about the dangers of the misuse of PCR testing. Perhaps not surprisingly, the video was removed from YouTube ‘for violating its terms of service’. After some digging, I found it posted on archive.org.
In the video, Mullis candidly states: ‘It’s just a process that is used to make a whole lot of something out of something. It doesn’t tell you that you are sick and it doesn’t tell you that the thing you ended up with was going to hurt you or anything like that.’
3. Fast-forward to January 7, 2020. Authorities in China’s Wuhan province announce that a novel coronavirus is the cause of cases of pneumonia detected around the end of December 2019.
Remarkably, only three days later, on January 10, a complete viral genome sequence is made available on virological.org.
4.Around this time in January, Professor Christian Drosten develops a RT (Reverse Transcription)-PCR test protocol for the novel RNA virus, SARS-Cov-2, in his lab in Berlin, based on Mullis’s PCR technique.Drosten’s testing protocol is accepted by the WHO on January 13, 2020.
This is almost two months before the World Health Organisation declares the novel coronavirus a pandemic on March 11, 2020.
On January 21, the Corman-Drosten paper is submitted to the journal Eurosurveillance. A rushed peer review occurs the following day (this peer review has never been released despite repeated requests from international scientists).
On January 23, the Corman-Drosten paper is published, laying the foundation for the RT-PCR test to be the ‘gold standard’ for detecting SARS-CoV-2, later confirmed by the WHO.
A sample of the authors of the research paper include: Victor M Corman, Christian Drosten (inventor of the PCR protocol for SAR-CoV-2 who also happens to be the editor of Eurosurveillance), Olfert Landt (CEO of the Tib-Moblbiol biotech company), Jenna Ellis (Public Health England scientist), Maria Zambon (a member of the Government scientific advisory body SAGE, of the New and Emerging Respiratory Virus Threats Advisory Group and of the WHO International Health Regulations emergency committee). I will refer back to these authors and their conflict of interests in Part 2 of my investigative report
5. The science journalist and geneticist Peter Andrews wrote an article in December 2020 about a proper peer review of the Corman-Drosten paper conducted by a group of 22 highly-experienced scientists from Europe, the USA and Japan.
The group comprised senior molecular geneticists, biochemists, immunologists and microbiologists. They found at least ten major flaws with the paper. The website of the independent peer reviewers is at CormanDrostenreview.com
Andrews highlights some of the major flaws of the Corman-Drosten PCR protocol, flagged by the 22 group peer review:
Non-specific, due to erroneous primer design.
Enormously variable.
Cannot discriminate between the whole virus and viral fragments.
Has no positive or negative controls.
Has no standard operating procedure.
Does not seem to have been properly peer-reviewed.
Dr Mike Yeadon, one of the scientists who was part of the international review group, highlighted another major flaw with the PCR test in ‘its propensity to suffer from contamination, and the integrity of a PCR is very easily destroyed by invisible levels of contamination even in the hands of an expert, working alone and on a small handful of samples’.
If only the failings of RT- PCR testing ended there. But, tragically, they don’t. The probability of a false positive result of Covid-19 arising from a PCR test is notably high, especially when a high cycle threshold (CT) value is used.
As I wrote earlier, the PCR test works by replicating strands of DNA or RNA in order for them to become large enough to identify. The number of cycles it takes to produce something identifiable is called the cycle threshold value. Anything above a CT value of 35 increases the chance of a false positive result.
Dr Andrew N Cohen co-authored a report as early as May 2020 warning of the dangers of false positive results generated from PCR testing. The research paper alarmingly states:
‘We derived a conservative estimate of the range of false positive rates that can reasonably be expected in SARS-CoV-2 testing. Findings: Review of external quality assessments revealed false positive rates of 0-16.7 per cent with an interquartile range of 0.8-4.0 per cent.’
This means if you are testing 30million people (approximately just under half population of the UK), using a conservative 1 per cent false positive rate it will result in 300,000 false positives.
If you take the median rate of 2.4 per cent, it results in 720,000 false positive cases. You can guess where I am going here – you’ve already got an epidemic just in false positive cases.
The paper goes on to state ‘the high false discovery rate that results, when prevalence is low, from false positive rates typical of RT-PCR assays of RNA viruses raises questions about the usefulness of mass testing; and indicates that across a broad range of likely prevalences, positive test results are more likely to be wrong than are negative results, contrary to public health advice about SARS-CoV-2 testing’.
6. The turning point in exposing the test’s unreliability came on November 20, 2020.An appeals court in Portugal made the monumental ruling that ‘the PCR process is not a reliable test for Sars-Cov-2, and therefore any enforced quarantine based on those test results is unlawful’.
The OffGuardianarticle reporting it stated: ‘In their ruling, judges Margarida Ramos de Almeida and Ana Paramés referred to several scientific studies. Most notably this study by Jaafar et al., which found that – when running PCR tests with 35 cycles or more – the accuracy dropped to three per cent, meaning up to 97 per cent of positive results could be false positives.’
7. On December 14, 2020 (many months after the unreliability of the PCR test was widely known and after thousands of false positive cases were counted as Covid cases**) the WHO finally issued a warning statement that using a high CT value would result in false positives**.
An extract from its statement warns: ‘When specimens return a high CT value, it means that many cycles were required to detect virus. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain’.
The report goes on to state that an ‘adjustment of the PCR positivity threshold is necessary to account for any background noise which may lead to a specimen with a high cycle threshold (CT) value result being interpreted as a positive result’.
(me: the insanity of testing aysmptomatic people with RT-PCR test only )
Dr Thomas Binder MD, one of the 22 authors of the external peer review (mentioned in Part 1 of my report) of the Corman-Drosten research paper tweeted: ‘It is madness to test with a hypersensitive unspecific RT-PCR test only, without consideration of CT & clinical findings. And it is the coronation of insanity to test even asymptomatic people in this way.’
Richard Tice (leader of Reform UK) was spot on when he said in his piece for TCW: ‘Stop testing the asymptomatic, stop wasting money and give people back the freedoms we need to get this country back working, living, educating, and loving again.’
The WHO’s technical data manager, Maria Van Kerkkhove during the organisation’s media briefing back in June 2020 stated: ‘Based on our data, it seems unlikely that an asymptomatic carrier will transmit the infection to someone else. We have a number of reports from other countries. They monitor asymptomatic carriers, their contacts, and do not detect further transmission.’
This was further confirmed in an article in the British Medical Journal by Professor Allyson Pollock, where she wrote: ‘A city-wide prevalence study of almost ten million people in Wuhan found no evidence of asymptomatic transmission.’
Dr Reiner Fuellmich explains in the youtube below that the PCR test created fear which was accompanied by measures which caused medical and economic disasters for millions.
I listened carefully to this and he failed to point out that much of the sickness and medical impact throughout 2020 and 2021 could be a combination of fear and stress creating an ideal environment for respiratory illness as well as medical errors and malpractice in failing to treat symptomatic patients with simple solutions discovered early on by many practicing clinicians. These impacts were of course severe in those with underlying illnesses and physical and mental weaknesses.
It is more than likely that there was a corona strain which affected many and was quickly resolved for most by the early use of HCQ zinc azithromycin or ivermectin in the appropriate dosage. Where the strain was allowed to go untreated it seemed to turn into a vascular disease where respiratory mechanical solutions just exacerbated problems, I think??!
The PCR test may not have any real benefit. If the experts in these articles are to be believed the false positives are so high as to make all tests worthless.
I wonder whether it’s possible to look at the data on 5 year average weekly deaths and actual weekly deaths per illness categories differently. Instead of saying all deaths in the 2nd wave described as covid deaths were not covid deaths but were in the 1st wave could we not say something differently. If one can take the plunge and say all testing is useless and should be ignored then the additional deaths need to be explained in the unusual period in April - May 2020 – and in winter months of November 2020 to March 2021:
Could it be that the yellow deaths are a combination of a small number of solely covid deaths due to medical malpractice in the main with some rare occurencies in younger people without comorbidities. But the majority were due to vascular related damage caused by the spike protein ( and not the actual virus) combined with the massive stress of lockdown, isolation, lack of normal social contact and economic harm. The timing would support this interpretation I think??! The data since vaccination began would of course show serious side effects but as yet not a massive death toll which could be because the virus was rarely encountered and a reaction was not triggered, whether this continues through the winter we shall see. The question remains how did this spike protein get into our system in 2020 – GOF manipulation and release either deliberately , recklessly or accidentally is the obvious answer. With of course all of the usual suspects in the frame.
This is just a layman’s view of the diverse information coming at us from all sides!
cheers
apologies if these links have been posted already.
The Drosten protocol, hijacked from Mullis’s PCR test, looks like it was cobbled together with surprising haste to lead us in a certain direction, simply ignoring the flaws that have been pointed out. Then other protocols were also breached as rushed ‘peer review’ unworthy of the name gave the process a shaky veneer. They and governments have been dodging criticism ever since.
It’s fertile legal ground for Fuellmich but I still wonder if he night need the treatment side to carry sway or the governments will be able to argue necessity in the face of whatever level of pandemic/epidemic is agreed on. Thanks for putting the story together.
From your comment highlighting the spike protein and vascular damage it’s clear you’re following the medical events!
You say: “I wonder whether it’s possible to look at the data on 5 year average weekly deaths and actual weekly deaths per illness categories differently. Instead of saying all deaths in the 2nd wave described as covid deaths were not covid deaths but were in the 1st wave could we not say something differently. If one can take the plunge and say all testing is useless and should be ignored then the additional deaths need to be explained in the unusual period in April - May 2020 – and in winter months of November 2020 to March 2021:”
Well when it’s misused I’d say it’s worse than useless - but it shouldn’t be completely useless if it’s used properly, to confirm a clinical suspicion of a disease. Or even worse, to become the definition of disease - diagnosed and used by bureaucracy.
My description of 1st wave ‘covid deaths’ leaves open the possibility that covid wasn’t the main cause for many of them. In the second wave the ‘yellow’ deaths below the 5-year average (dotted line in the graph further up) should be considered not covid-related at all. To me this takes criticism of the PCR test as far as I can without knowing more about the role played by covid in the deaths in the 1st wave; this also applies to the ‘covid-deaths’ in the 2nd wave that are above the dotted line, hence probably influenced by covid - unlike their below the line counterparts.
You: "Could it be that the yellow deaths are a combination of a small number of solely covid deaths due to medical malpractice in the main with some rare occurencies in younger people without comorbidities. But the majority were due to vascular related damage caused by the spike protein ( and not the actual virus) combined with the massive stress of lockdown, isolation, lack of normal social contact and economic harm. The timing would support this interpretation I think??! The data since vaccination began would of course show serious side effects but as yet not a massive death toll which could be because the virus was rarely encountered and a reaction was not triggered, whether this continues through the winter we shall see. The question remains how did this spike protein get into our system in 2020 – GOF manipulation and release either deliberately , recklessly or accidentally is the obvious answer. With of course all of the usual suspects in the frame."
Well I think there’s been malpractice throughout in not treating the early virus stage, and also outrages relating to PPE and dumping old people with covid into care homes (probably some of the use of ventilators was wrong but wouldn’t qualify as malpractice if it was thought to be right).
I don’t think that’s what you mean though - there’s a school of thought that says the spike protein itself causes injury, but isn’t that still covid injury? Are you bringing in vaccine spike proteins here - but they weren’t around early enough to have caused the deaths in the so-called (edit) third second wave. Undoubtedly there are lockdown deaths and economic deaths, there’s no quantification yet. Maybe I’ve picked you up wrongly…(or maybe we need to bring in evidence from the Socialist Man! )
Though if you just look at excess deaths you could make a case that all the excess deaths are through malpractice or mismanagement but I think this would be political rather than medical or legal (?).
Leaving in covid as a factor (even with the misused PCR) at least allows one to say that covid didn’t explain all the deaths in the second wave.
Cheers
Yes very many thanks for all this background info on the PCR, and particularly on Christian Drosten’s involvement in the Reverse Transcriptase part of it, of which I was unaware. This is specially significant because Drosten is a key figure in the Plandemic, being a signatory to Peter Drazsak’s letter to the Lancet of ?28th January. His association with the Ecohealth alliance as well as with the Charite hospital in Berlin makes him some sort of German Fauci, IMO.
I accept all the logic in these contributions and your broad conclusions - which I have only skimmed through and will study further later.
In Victoria we are now plunged into a 7 day lockdown due to an outbreak that has so far affected 30 people, but as usual with 40,000 people from “exposure sites” tested and only three positive cases. Somehow in Australia where there is no virus the tests don’t show false positives at all. I never found out if they are only doing 25 cycle tests so as to be sure there are no false positives… or whether there aren’t actually any cases at all and the whole story about escapes from quarantine, which always happen just before public holidays and weekends so as to cause maximum pain and loss, may be a lie.
But it works! People are now rushing to get their poison stabs, worried out of their wits about this invisible plague that could strike them down in the street. No-one has died from CV for six months, and none of the recent alleged cases has ended up in hospital. Though we don’t know who they are, and couldn’t find out.
Now it’s the Indian Variant, more infectious and deadly and spreading wildly, so we must all mask up and be alarmed… strewth. ZERO opposition to this in media or public debate.
Dead right. And of course, it was Fauci’s NIH money that funded the Ecohealth alliance (along with Kill Gates) that then funded the Wuhan lab doing gain of function! Drazsak is in it up to his neck, along with all the others.
Ha ha ha! Didn’t that get absorbed into the New Statesman during those long years of morphing into the New Statesman & Society and then back again? (Yes, I was a reader. The one good consequence was that Paul Sieveking’s column led me to Fortean Times and from there down way too many rabbit holes)
Reading all of the above it surely is patently obvious that RT-PCR is a busted flush? Pardon the pun but this leads me to believe that the water assays being made at sewage plants may be the new way to delineate CronyVirus hot spots. Marvellously vague, wholly unattributable, and (un)intentionally hilarious.
Really the whole thing is just a Cop who pats you down and says “Now then sonny, what’s this I’ve found in your coat pocket…?”
Over the years I’ve tended to glean what I could from gazing down the rabbit holes from above without taking the plunge, but we may be in a rabbit grand canyon that has leapt on top of us.
The trouble is that the busted flush, the PCR tool, is still being happily misused and accepted.
Hi @Evvy_dense ,
I think what I am trying to say is something that has been around for almost a 150 years - the Terrain is everything and the Germ is nothing ( or not much ) - examined here:
if we follow this principal and look at what has happened to the terrain (our minds and bodies) over the last 17 months, chronic stress has been imposed on everyone to a massive degree. If we apply and adapt Cohen’s question as to whether his 35 years of research on chronic stress to other respiratory diseases can be applied to coronavirus then we can perhaps understand why we had the April to June 2020 impact. ( for the 2nd wave in November 2020 it is the usual season for illnesses and Cohen’s remarks would not need to be adapted they would be totally on point)
Merely saying stress kills people with respiratory illnesses does not explain the totally unusual events of April to June 2020 - I think commentators say this has never happened before. But if we regard the illness as a combination of a spike protein generated vascular disease and chronic stress this may not operate in the same cyclical manner as respiratory diseases and could explain the timing later in May of the year. When these 2 elements combine to attack an already weakened terrain then without the available treatments deaths occur.
I could of course be way out on this spike thing. It maybe that this is just a quirk of the new coronavirus. But it seems to me that the generation of chronic stress through the deliberate policy of fear mongering in everyone over 2020-2021 could easily have been the direct cause of so many deaths. I also understand that scientists have known about these spikes for decades in other virus’ except these have not produced anything similar in terms of vascular damage, afaik. So this is another reason why we should look closely at terrain theory and recognise what these SICs have done to the terrain of the global population!
" I could of course be way out on this spike thing. "
Well it’s at the scene of the crime - almost caught red-handed…a post by @Robg earlier this month reported that researchers have used a ‘pseudovirus’ containing just synthetically-created spike proteins and showed the spike proteins damaged cells by binding to ACE2 - just as the Sars-cov2 spike protein does - but without needing any more ‘virus’ than that.
Terrain - recent history, gain of function? It is looking very possible that the spike was created deliberately to make a new virus more replicative. Dr Richard Fleming asserts this very pointedly Vaccines Have Zero Efficacy and May Cause Mad Cow Disease – GNEWS based on the research of the ‘Batwoman’ Zheng Shi.
[I don’t get this claim he makes that vaccines have zero efficacy though]
I would also agree that germs need to be considered along with the state of the system (body) in which they reside. Alternative health practitioners have been saying this for over a decade and I think there are indications that the ‘medical world’ is slowly coming round to that view. I wouldn’t dispute that the direct effects of stress on the gut are part of that system.
Did the stress of everything play a big part in the spike in deaths last spring?
I believe stress has been a factor in covid deaths. I saw a study to this effect somewhere. It’s discussed here
so it’s certainly not impossible. Granted, the countries with big first waves (rich Europe, the US) were the ones whose governments put their populations through hoops causing panic. I wouldn’t have thought it was the reason for the shape (spike in deaths) though, as there appeared to be spikes in other countries. I’d also expect it to affect people without covid but with other illnesses, if so that would flatten any spike. Many countries spiking recently in Eastern Europe had little in the way of first waves and some have overtaken rich Europe. But without knowing more about the stresses and how they played out, I wouldn’t rule it out!
Interesting to note that the Vox article lays such emphasis on societal stressors (many you’d have missed entirely if disconnected from internet and the idiot box).
As you say @Evvy_dense, the amplifying (if not directly seeded) effects of meeja-political ideological apparatus must have been influential, but something else was going on the background.
I’ve only dipped in and out of this book by Gabor Mate but it has some telling points to make as regards ‘terrain’.



 )
)