Dr Cremola’s article (pasted below) will vanish before tomorrow morning, cruelly pulled by the all-the-year-round GGIC’s (Gangster Grinches in Charge, trying to ruin 365 days of each year) though I think the video will survive on BrandNewTube. It’s a mere 2hr 45m!
He’s made the big time - the Joe Rogan podcast! It apparently has one of the biggest reaches in podcastium.
From his beginning in covid treatments, McCullough’s view has hardened.
" “It seems to me, early on, there was an intentional, very comprehensive suppression of early treatment in order to promote fear, suffering, isolation, hospitalization and death. And it seemed to be completely organized and intentional in order to create acceptance for and then promote mass ‘vaccination.’”
Some more that Dr Cremola has highlighted:
“Robert Kennedy Jr.'s book, “The Real Anthony Fauci” also shows, using extensive documentation, that Moderna was working on an mRNA injection for COVID-19 well before the world even knew it existed. He reveals extensive collusion occurred to push this novel gene transfer technology on the world, with devastating effects.”
(ED - this is a key fact worth checking as it’s probably of “smoking gun” prortions, especially given Moderna’s little-known DoD origins)
“After intense pressure to produce evidence of reinfection, the U.S. Centers for Disease Control and Prevention finally admitted they don’t have a single verified case of someone getting sick with COVID twice.”
(ED: McCullough puts the reports of re-infections down to the vagaries of PCR testing with high Ct value. Interestingly, Dr Robert Malone disagrees…)
"Historically, any drug with five unexplained deaths gets a black box warning. At 50 unresolved deaths, it’s pulled from the market altogether. None of that happened here. To this day, the FDA and CDC claim not a single death is attributable to the COVID shots, even as the reported death toll is nearing 20,00012 (including international reports), with half of them occurring within 48 hours of the injection. Eighty percent occur within a week post-injection.
That is simply unheard of. The temporal association is stronger than anything we’ve seen before. McCullough also cites research concluding that in 86% of cases, there was no other explanation for the death other than the COVID shot."
“Interestingly, the shots appear to harm men and women differently. Women are having far higher rates of neurological injuries, whereas boys and young men account for some 80% of myocarditis (heart inflammation). Just how bad is the myocarditis wave?”
Reject Boosters
"If you’ve taken one or two COVID jabs months ago and nothing bad happened, count your blessings. You’re among the lucky ones. If you persist in taking boosters, however, your luck is probably going to run out at some point. It’s really only a matter of time before the amount of spike protein in your system overwhelms it, producing noticeable damage.
Again, evidence suggests the spike protein may remain for 15 months post-injection. McCullough believes it will last at least a year after each dose. If you start getting boosters every three to six months, you’re never going to get rid of that spike protein."
(ED: Given the Spike Protein is reputed to to most of the damage, this is perhaps another key point:
“If you fear COVID-19, you ought to be just as fearful of the COVID shots, if not more so, as you end up with far more spike protein from the shot than you do from the natural infection.”)
Video link: https://brandnewtube.com/themes/youplay/player/css/mejs-controls.svg
ED
The Most Important Podcast You Can Hear About COVID-19
Analysis by Dr. Joseph Mercola
Story at-a-glance
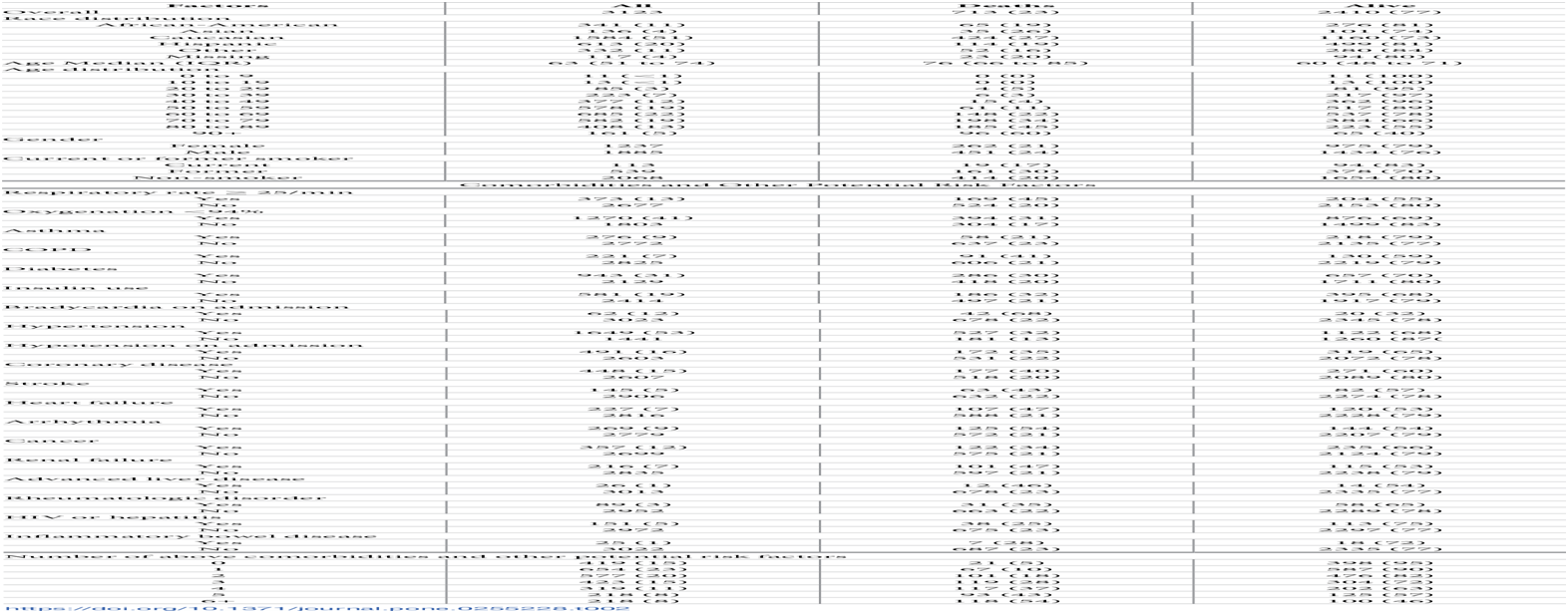
- Of the COVID-19 deaths in the U.S., none received adequate and/or early-enough treatment. At least 85% of COVID deaths were preventable
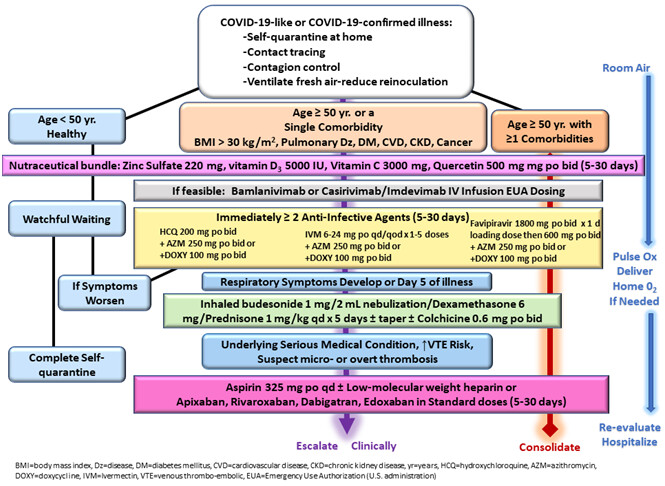
- There are three components to SARS-CoV-2 infection: viral replication, cytokine storm and blood clotting, therefore necessitating a multidrug approach, and treatment must begin early to be effective
- Research published in 2006 showed hydroxychloroquine reduced viral replication of SARS-CoV-1 (the original SARS virus). It also has well-established anti-inflammatory properties. These two properties help explain its usefulness against COVID-19
- There were clear intentional efforts to prevent use of hydroxychloroquine against COVID-19, likely in an effort to make the COVID jabs appear necessary
- You cannot get COVID-19 twice; those with natural immunity have robust, long-lasting immunity. The Pfizer COVID shot, meanwhile, has been shown to have undetectable effectiveness 201 days after the second dose and Moderna’s effectiveness reaches zero around day 121
If you could only listen to one podcast to get up to speed on COVD-19, you are in luck as one of the top clinicians in the world on understanding COVID-19, Dr. Peter McCullough, finally made his way to the largest podcast in the world, Joe Rogan and, as expected, it was epic. You will do yourself a serious disservice if you don’t watch the entire, nearly three-hour, interview at normal speed.
McCullough is an internist, cardiologist and epidemiologist, and in this podcast, he reviews and summarizes what we know about the COVID jabs. McCullough also discusses the importance of early treatment, which has been universally suppressed and ignored from the start.
He’s convinced, and states unequivocally in this interview, that of the COVID-19 deaths in the U.S., none received adequate and/or early-enough treatment. In short, people did not, and certainly don’t now, need to die from this infection, barring some serious underlying condition.
It’s treatable, and later variants, such as Delta and Omicron, appear generally milder than the original virus, resulting in even easier-to-treat illness. From early on, researchers and clinicians demonstrated that early treatment, be it with hydroxychloroquine, ivermectin or steroids and anticoagulants — in some combination — resulted in far better outcomes and saved lives.
When you just let the infection run its course without treatment, most COVID-19 patients were riddled with blood clots and other complications by the time they were hospitalized. According to McCullough, we know that at least 85% of all COVID deaths could have been avoided with early treatment.
Early Treatment Is Key
In August 2020, McCullough’s landmark paper “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection” was published online in the American Journal of Medicine.1
It was the first published report on how to treat COVID on an outpatient basis and described a comprehensive COVID treatment protocol for frontline doctors. Before this, there were about 4,000 papers discussing the potential benefit of various remedies, but none that actually sought to present a comprehensive protocol for treatment.
A follow-up paper, “Multifaceted Highly Targeted Sequential Multidrug Treatment of Early Ambulatory High-Risk SARS-CoV-2 Infection (COVID-19)” published in Reviews in Cardiovascular Medicine in December 2020,2 became the basis for an AAPS home treatment guide.
Importantly, McCullough and the team of collaborators he put together understood early on that there were three components to this infection: viral replication, cytokine storm and blood clotting, therefore necessitating a multidrug approach.
One drug that gained early attention was hydroxychloroquine, as research published in 2006 showed it reduced viral replication of SARS-CoV-1 (the original SARS virus). It also has well-established anti-inflammatory properties. It’s been routinely used in the treatment of lupus, for example. But as explained by McCullough, there were clear intentional efforts to prevent use of the drug against COVID-19.
The U.S. government refused to release its stockpiles, and doctors were told they’d lose their medical license if they used it. The largest manufacturing plant of hydroxychloroquine even mysteriously burned down, and in South Africa, “mercenaries” were breaking into pharmacies and burning the drug.
In addition to that, a fraudulent paper was published in the journal Lancet, falsely stating that hydroxychloroquine was dangerous. “It looked like it was a step to bury hydroxychloroquine as a treatment,” McCullough says. When focus shifted to ivermectin, that drug also became inaccessible and was widely vilified as “horse paste” in the mainstream media.
Treatment Was Suppressed for a Reason
Considering the overwhelming success doctors have had in treating the infection with these and other drugs, why aren’t hospitals everywhere doing it? Why have health authorities fought against treatment in general, and the use of hydroxychloroquine and ivermectin in particular? In McCullough’s words:
“It seems to me, early on, there was an intentional, very comprehensive suppression of early treatment in order to promote fear, suffering, isolation, hospitalization and death. And it seemed to be completely organized and intentional in order to create acceptance for and then promote mass ‘vaccination.’”
The plan to create acceptance for novel mRNA gene transfer technology in lieu of a conventional vaccine by suppressing treatment options has been explained in detail in Dr. Peter Breggin’s book, "COVID-19 and the Global Predators: We Are the Prey,"3 and Pamela Popper’s book, "COVID Operation: What Happened, Why It Happened and What’s Next."4 McCullough recommends both, if you want to understand how this was coordinated and planned.
Robert Kennedy Jr.'s book, “The Real Anthony Fauci” also shows, using extensive documentation, that Moderna was working on an mRNA injection for COVID-19 well before the world even knew it existed. He reveals extensive collusion occurred to push this novel gene transfer technology on the world, with devastating effects.
When asked why more doctors aren’t using these early treatment protocols, McCullough points out that of the 1 million or so doctors in the U.S., probably only 500 or so actually understand that viable treatments are being suppressed with the intent to drive uptake of the gene transfer shots. Those relatively few who do understand what’s going on face censorship and the threat of having their medical license removed if they speak out about treatment.
Questions About Reinfection Linger
A widespread concern that Rogan brings up is whether or not you can actually get COVID twice. According to McCullough, the answer is a hard no. You cannot. You might think you have it twice, because you’ve tested positive.
After intense pressure to produce evidence of reinfection, the U.S. Centers for Disease Control and Prevention finally admitted they don’t have a single verified case of someone getting sick with COVID twice.
To prove reinfection, McCullough says, you’d need to have a positive PCR test at a cycle threshold below 28 (not 40 or 45, as is routinely done), and a positive antigen immunoassay test to show that you actually had antibodies from the first infection, and a gene sequencing test showing you in fact have the SARS-CoV-2 virus.
What’s more, dozens of studies confirm that natural immunity is robust and long-lasting. “So why is there so much resistance to the idea that people have natural immunity?” Rogan asks, to which McCullough replies, “All roads lead to the ‘vaccine.’”
Dr. Robert Malone disagrees with McCullough on this issue, pointing to a December 4, 2021, study showing 12% out of a sample of 1,200 individuals experienced COVID reinfection.5 In a Twitter post, Malone said:6
“I have caught it twice, as has my wife. I was asymptomatic, she was not. This is a rapidly mutating RNA virus. Just like the common cold. The symptoms will not be as severe — but yes, people catch it more than once. Even Delta …”
Relative Versus Absolute Risk Reduction
Now, when it comes to the efficacy of these COVID shots, the manufacturers have employed a classic strategy to mislead the masses and make the shots sound far better than they actually are. That strategy is looking at relative risk reduction rather than absolute risk reduction.
While the COVID shots boasted efficacy rates between 67% and 95% at the outset, those were the relative risk reductions. The four available COVID shots in the U.S. provide an absolute risk reduction between just 0.7% and 1.3%.7,8
Now, compare that to the noninstitutionalized infection fatality ratio across age groups, which is 0.26%.9 Since the absolute risk that needs to be overcome is lower than the absolute risk reduction these injections can provide, mass vaccination simply cannot have a favorable impact. Yet here we are, being told to get used to the idea of getting booster shots at ever-increasing intervals. It just doesn’t add up.
Of course, as I’ve reported on several occasions, research and clinical experience clearly show that the effectiveness of these shots rapidly wanes. Six months after the second dose, your protection is nil. Meanwhile, your body continues producing toxic spike protein for at least 15 months after each dose.
Efficacy Rapidly Wanes
McCullough cites a Swedish study10 published October 25, 2021, which looked at data from 842,974 pairs, where each person who had received two COVID jabs was paired and compared against an unvaccinated individual, to see if the vaccinated had fewer symptomatic cases and hospitalizations.
Early on, the double-jabbed appeared to have good protection, but that quickly changed. The Pfizer jab went from 92% effectiveness at Day 15 through 30, to 47% at Day 121 through 180, and zero from Day 201 onward. The Moderna shot had a similar trajectory, being estimated at 59% from Day 181 onward. The AstraZeneca injection had a lower effectiveness out of the gate, waned faster than the mRNA shots, and had no detectable effectiveness as of Day 121.
All the while, millions of Americans have already had COVID11 and have natural immunity that doesn’t wane in this manner. Yet they are being shunned and fired for not complying with COVID jab mandates. Again, it just doesn’t add up. Never before has a vaccine been required for anyone with natural immunity against a disease, and there’s good reason for that. It’s completely illogical.
Just like you don’t need a measles vaccine if you’ve had measles, you don’t need a COVID shot if you’ve had COVID. In fact, you are at increased risk of adverse events if you do take it. Remember, if you already have natural immunity, you’re exposing yourself to the harms of the shot with no hope of benefit.
The Most Dangerous Injections in Medical History
As explained in this interview, the COVID shots are the most dangerous, most lethal drugs ever used — and the U.S. Food and Drug Administration and CDC knew this as early as mid-February, when the deaths reported to the U.S. Vaccine Adverse Events Reporting System (VAERS) hit 182.
Historically, any drug with five unexplained deaths gets a black box warning. At 50 unresolved deaths, it’s pulled from the market altogether. None of that happened here. To this day, the FDA and CDC claim not a single death is attributable to the COVID shots, even as the reported death toll is nearing 20,00012 (including international reports), with half of them occurring within 48 hours of the injection. Eighty percent occur within a week post-injection.
That is simply unheard of. The temporal association is stronger than anything we’ve seen before. McCullough also cites research concluding that in 86% of cases, there was no other explanation for the death other than the COVID shot.
McCullough points out that in any given year, an average of 150 deaths following vaccination are reported to VAERS. That’s 150 deaths from an average of 278 million vaccine doses given.
Here, we had 182 deaths at a point in time when only 27 million doses had been administered. So, you cannot blame it on the volume of shots given. The same trends can be found in other countries’ databases as well, such as the U.K.'s Yellow Card scheme.
What’s more, vaccine side effects are notoriously underreported, so as staggering as the VAERS data are, they’re just the tip of the iceberg. Historically, only 1%13 to 10%14 of adverse effects are reported. For the COVID shots, the underreporting factor has been calculated to be anywhere between 31 and 100. That means that to get a more accurate range, you have to multiply the VAERS number by 31 and 100.
The absolute most-conservative estimate so far is an underreporting factor of five. That estimate came from an FDA whistleblower who used Centers for Medicare and Medicaid Services data to estimate the underreporting in VAERS.15 According to that whistleblower, the number of Americans killed by the shots was at least 45,000 as of July 9, 2021. At that time, VAERS reported 9,048 deaths following COVID injection.
Who’s at Greatest Risk for COVID Jab Side Effects?
As explained by McCullough, one of the reasons for this massive death toll is the fact that the COVID shot introduces an uncontrolled dose of spike protein into your body — a far greater dose than what you get when naturally infected with the virus. And the spike protein is the most lethal part of the virus. It’s responsible for the most problematic symptoms of infection.
So, the shots are killing the same people that would be in dire straits were they infected by the virus. It’s also killing some who would likely fare OK with the wild virus but cannot handle the excessive spike protein load produced by the COVID shot.
Consistent Data Point to Clear and Present Danger
As noted by McCullough, we have a very clear safety signal from VAERS. We also have clear biological plausibility, meaning we can explain why and how people might be harmed by these shots. The data are also internally and externally consistent, within VAERS and databases in other countries. The same patterns are seen everywhere.
Normally association does not mean causality unless very specific criteria are met, and in the case of the COVID jabs, those criteria are indeed met. “We’ve fulfilled what’s called the Bradford Hill criteria for causality,” McCullough says. In other words, we have evidence that the injuries and deaths are not accidental. The COVID shots are indeed injuring and killing people at unprecedented rates, despite what the lying CDC states.
Myocarditis Will Likely Be Widespread
“Interestingly, the shots appear to harm men and women differently. Women are having far higher rates of neurological injuries, whereas boys and young men account for some 80% of myocarditis (heart inflammation). Just how bad is the myocarditis wave?”
“Research published in 201716 calculated the background rate of myocarditis in children and youth, showing it occurs at a rate of four cases per million per year. Assuming there are 60 million American children, the background rate for myocarditis would be 240 cases a year.”
“How many cases of myocarditis have been reported to VAERS following COVID injection so far? 16,918 as of December 3, 2021,17 and it’s going up by several hundred to a couple of thousand every week. We’re also seeing myocarditis in adult men.”
My fear is, some of these kids who develop myocarditis will be in the 13% category where they have progressive left ventricle dysfunction and heart failure. ~ Dr. Peter McCullough
“Doctors have never seen so many cases of myocarditis,” McCullough says. “It is frequent, and it is severe.” Patients require heart medication, and must remain sedentary for extended periods of time. While myocarditis is typically a nonfatal adverse event, it can shave years off your life.
“Research published in 2019 showed 13% of myocarditis cases ends up with progressive heart failure. Their hearts just never fully recover from the damage. In the study, another 36% improved but never fully recovered.”
“My fear is, some of these kids who develop myocarditis will be in the 13% category where they have progressive left ventricle dysfunction and heart failure,” McCullough says.
"While we don’t yet know exactly how COVID jab myocarditis compares to naturally-occurring myocarditis, the data we currently have suggest the damage incurred by the spike protein is rather severe.
According to McCullough, 86% of youth who develop myocarditis in response to the jab are sick enough to require hospitalization. Research also shows young boys are far more likely to be hospitalized with myocarditis than they are being hospitalized with COVID-19, McCullough says."
Reject Boosters
"If you’ve taken one or two COVID jabs months ago and nothing bad happened, count your blessings. You’re among the lucky ones. If you persist in taking boosters, however, your luck is probably going to run out at some point. It’s really only a matter of time before the amount of spike protein in your system overwhelms it, producing noticeable damage.
Again, evidence suggests the spike protein may remain for 15 months post-injection. McCullough believes it will last at least a year after each dose. If you start getting boosters every three to six months, you’re never going to get rid of that spike protein.
You’ll be adding more and more with each dose, and it’s the same spike protein that causes problems in COVID-19. If you fear COVID-19, you ought to be just as fearful of the COVID shots, if not more so, as you end up with far more spike protein from the shot than you do from the natural infection.
At this point in time, the evidence is clearly weighing against the COVID shots. They’re causing far more harm than good, especially among children, who are not at high risk of dying from COVID-19 in the first place."
Sources and References
- 1 American Journal of Medicine January 2021; 134(1): 16-22
- 2 Reviews in Cardiovascular Medicine 2020; 21(4): 517-530
- 3 COVID-19 and the Global Predators: We Are the Prey by Peter Breggin
- 4 COVID Operation: What Happened, Why It Happened and What’s Next by Pamela Popper
- 5 medRxiv December 4, 2021; 2021.07.20.21260855
- 6 Twitter Robert Malone December 16, 2021
- 7 Medicina 2021; 57: 199
- 8 The Lancet Microbe July 1, 2021; 2(7): E279-E280
- 9 Annals of Internal Medicine September 2, 2020 DOI: 10.7326/M20-5352
- 10 Lancet Preprints October 25, 2021
- 11 Our World in Data December 15, 2021
- 12 OpenVAERS December 3, 2021
- 13 The Vaccine Reaction January 9, 2020
- 14 BMJ 2005;330:433
- 15 US District Court for the Northern District of Alabama Civil Action No: 2: 21-cv-00702-CLM (PDF)
- 16 Journal of the American Heart Association November 18, 2017; 6:e005306
- 17 OpenVAERS Adverse Events Reports as of November 19, 2021

{kind=link}