I find this almost unbelievable from an intelligent guy, and I assume it’s not sarcasm? I suggest you do two things to debunk (or reverse) your opinion. Vaccine Canada did an excellent analysis of the PCR “test” including using the test manufacturer’s own figures. When you’ve watched that, find out:
a) Who supplies the primers for the UK test
b) How many cycles are they using
If you still are not convinced, then we’ll have to agree to disagree.
Thanks @PatB I’ll take a look. So far I’ve seen lots of theoretical worries about false positive results, but zero examples in the real world. On the other hand I’ve seen several mass testing exercises that have shown zero positive results or very tiny numbers. How does one get zero positives out of 10 million tests if false positives are a really big thing?
If false positives were a serious real (as opposed to theoretical) problem then I would have expected more evidence of that in the mass testing that has been done…
As always, I’m very open to data showing otherwise. I’m always happy to consider that I might be dead wrong.
Hi, Pontius. I’m intrigued by your confidence in a PCR test. It has been criticised, not because it is a flawed test, but that it can be misused so readily by cycling the test sample multiple times to pick up even dead virus debris. This positive test is then used, politically, to use the measures that we are living under now. You don’t need to be on Twitter to read tweets, so I hope you will have a look at some of the criticisms of the PCR test (and some insight of Bayes Theorem too!) here…
Yes, I get this and it is convincing in theory. In the real world data I’ve seen, there have been several examples of a population that gets a lot of tests (10 million at a time, for example) but produces zero or close to zero positive results…
If there were a lot of false positives we should never see that. There should always be a set number of positives, never zero. Similarly, the trends (upwards and downwards) of cases were pretty close to that of the ZOE covid symptom tracker (at least for the period when I was paying attention). ZOE had pretty good agreement with the ONS too, which uses PCR. That means that for all it’s problems, cases as measured by PCR agreed with cases as measured by self reporting symptoms through an app. Again, this should not happen if one measure (PCR) is horrible biased.
You go on to say
and I completely agree with that. This makes everything more complex because presumably this is something that can be dialled up or down depending what the political need is. That is politicians could direct labs to use more or less cycles depending what outcome they want.
I’m very willing to admit that this could be happening. Is it definitely happening? I don’t know.
Thanks for the links and tweets. Bayes’ theorem is definitely the correct way to think about this, but I’ll need a fresher head than I have right now to go through it
Morning, Pontius, and everyone here too, of course!
A “fresher head” is a must to follow the Bayes Theorem, and indeed, why the difficulties of mass testing by laboratory tests done quickly and accurately is so very hard to achieve:
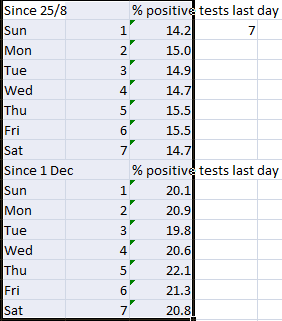
" Dr Craig: There’s a beautiful piece of evidence that’s just been produced by a physicist in Scotland called Christine Padgham, who is a force of nature and has gone carefully through all of the Scottish data. Public Health Scotland have been much more open with the data that they’re publishing, and they include in their publications the daily positive numbers, the daily negative numbers, the total number of tests done, and so you can actually get a percentage of positive tests per day that’s accurate. And when you look at the percentage of positive tests per day in Scotland, the percentage of positives is twice as high at the weekends than it is on a Monday. Now that cannot be anything to do with the disease.
That’s to do with the laboratories being under extraordinary pressures. It’s to do with people. The PCR testing, which is the test that we use for COVID, can be an incredibly specific test with a low false positive rate, but it can also be incredibly difficult to actually do because the first step is to translate your RNA to DNA and then you double the amount of DNA in the sample. You double it, and you double it, and you double it until you’re at a billion or a trillion times the amount you began with. What that means is that even the tiniest, tiniest amount of cross-contamination from other things in the lab can mean that you get the wrong result.
Whenever you run a test, you’re going to definitely put a certain positive in that test so you can make sure that the test worked properly. Every time they run a test, a positive control sample is being used. And if a little bit of RNA from that sample gets onto a glove, and gets onto the fridge door or something else around the lab, then every person that touches that fridge door is going to get contaminated, and the samples that they touch will get contaminated. The difference between a weekend and a Monday in a lab is that at the weekend you’re short-staffed, and people are tired, and the labs had all the problems that built up over the week hanging over. On a Monday, people come in fresh-faced. They’ve had a rest over the weekend, and the lab is thoroughly cleaned, and then you get out new chemicals that are all brand new and clean, and you start again."
“Follow” her, if you can, on Twitter, she is a star!
I appreciate the idea and the scepticism, definitely going to check out these two professionals-with-independently-functioning-brains.
What a nice idea - but is it true? I couldn’t get it to agree.
Those making the pcr test the standard have a lot to answer for. However pcr-positives will still include the real infections amongst the ones that aren’t real. I presume this will still be true irrespective of the possibility of contamination.
There are few false positives in the sense of the sars2 not being present at all - but there will be many that are false in the sense of the person not having a clinical infection.
‘They’ babble on about the number of ‘cases’ or ‘infections’ or ‘people who are infected’ when most probably are not. This has helped create a culture of ‘the Vaccine will save our normal lives’, and ‘HOW can I get the vaccine quicker’. etc.
A proportion of people get a positive PCR with a high Ct value and are obliged to self isolate because, not being told their Ct number, are not aware they are not actually infected or infectious.
The number of cases is open to external influence just by tweaking the number of Ct cycles. It may have been you Bob who posted (was it?) that the WHO were now advising bringing the Ct number down, and observing that this would reduce ‘cases’ timeously with the vaccine roll-out.
Pcr is fraught and should not be the sole driver of policy, I hope someone get to the bottom of it!
With you here RG - as here in CV-free OZ the hospital crisis is overwhelming us, along with endless talk of vaccines. I believe nothing I hear from mainstream media any more, if it conflicts with what I KNOW. And the one thing I do know, is that were HCQ+ to have been used generally, and still could be, then we would never have had this crisis of people ending up in hospital, nor the same spread of the virus, except perhaps amongst the old and sick.
Much more to say on this, when I have time. Every day in Australia there are at least 25,000 tests done, with NOT ONE positive case found. Doesn’t add up. And sometimes they expose themselves. Today it was announced that “fragments of virus have been found in waste water” in three country towns each 100 miles apart where there have never been more than one or two cases, so anyone living there or who has visited recently should get tested “if they have even the mildest of symptoms”. The reason they came up with this, after a fortnight without a single positive case, is because tonight the emergency state was due to lapse. It has now been renewed for another month. Case proven, they lied!
Thanks @Bob_sYourUncle - both posts with excellent content that I’ve now read. It inspired a lot of thoughts that I want to expand on, but it might not be today. I’ll follow up with you soon on the points you raise.
@Evvy_dense - some very good points there too. I think I’ll pick up my earlier thought about writing a more full post on some of my thoughts about PCR and false positives etc.
Exactly @Dimac - that is precisely the point I was making above. Zero false positives. I see that pattern all over the place, which makes me doubt the severity of the false positive problem in the real world. And I started off believing that it would be a real problem as we ramped up testing.
Pontius and Dimac, if there really is 25,000 tests being done without a single positive result, we can be sure it’s not real!
The PCR test, like all tests have a percentage that will return a false result, the more accurate the test (and the tester!) the closer the result will be to 100% accuracy.
An old post from Mike Yeadon but, I hope, will have lost nothing by this:
“Think of any diagnostic test a doctor might use on you. The ideal diagnostic test correctly confirms all who have the disease and never wrongly indicates that healthy people have the disease. There is no such test. All tests have some degree of weakness in generating false positives. The important thing is to know how often this happens, and this is called the false positive rate. If 1 in 100 disease-free samples are wrongly coming up positive, the disease is not present, we call that a 1% false positive rate. The actual or operational false positive rate differs, sometimes substantially, under different settings, technical operators, detection methods and equipment. I’m focusing solely on the false positive rate in Pillar 2, because most people do not have the virus (recently around 1 in 1000 people and earlier in summer it was around 1 in 2000 people). It is when the amount of disease, its so-called prevalence, is low that any amount of a false positive rate can be a major problem. This problem can be so severe that unless changes are made, the test is hopelessly unsuitable to the job asked of it. In this case, the test in Pillar 2 was and remains charged with the job of identifying people with the virus, yet as I will show, it is unable to do so.”
“So, what is the false positive rate of testing in Pillar 2 [Testing in the community]? For months, this has been a concern. It appears that it isn’t known, even though as I’ve mentioned, you absolutely need to know it in order to work out whether the diagnostic test has any value! What do we know about the false positive rate? Well, we do know that the Government’s own scientists were very concerned about it, and a report on this problem was sent to SAGE dated June 3rd 2020. I quote: “Unless we understand the operational false positive rate of the UK’s RT-PCR testing system, we risk over-estimating the COVID-19 incidence, the demand on track and trace and the extent of asymptomatic infection”. In that same report, the authors helpfully listed the lowest to highest false positive rate of dozens of tests using the same technology. The lowest value for false positive rate was 0.8%.”
I hope that this helps in understanding any country (China was mentioned earlier, and now Australia) that are conducting these tests and getting zero positives, are:
a) Not testing!
b) Lying about the tests that are being done!
PP. Don’t know how many times I have already said this but I am going to say it again!
Zero positives (false or true) is easy to manage. Change the primer used on the PCR, or, reduce the cycles!! Then, when “they” want to up the lockdown and/or fear, up the cycles and hey presto, the number of positives will reappear. And the more cycles, the more false positives.
As Kary Mullis said (and its well documented), with PCR, "you can find anything in anyone". It doesn’t mean they are sick, or contagious.
I know it’s possible. Is that what they’re doing, though? I’d like to see some evidence.
How does this work, though?
In Oz they justify having a lockdown by running the PCR cycles down to reduce cases.
In the UK that justify having a lockdown by running the PCR cycles up to increase cases.
Heads you win, tails I lose.
It’s possible. An alternative hypothesis is that the specificity of the test is good enough to avoid 1 false case in 25,000 tests. This is fairly consistent with what the ONS found in the UK too. And in China as well.
I think there is a lot of confusion about what false positives are and how serious they are. I’ll try and write some more about it soon.
You got me wrong PP - as others below are noting. My observation on the absence of positive tests in Victoria was that this was scientifically impossible as well as verifying the fabrications and falsification of all the testing and claims about Coronavirus presence and absence. If you were to do any test and find no positives in 25,000 samples then you would conclude, regardless of what the test was, that there was a fault in the equipment so all the results were invalid - there are ALWAYS false positives. But NOONE EVER points out this problem! Anymore than anyone ever suggests that testing of so many positive cases in Europe could be inaccurate or exaggerated or underestimated. This is SCIENCE!!!
In fact in Victoria, in its spell of 70 odd days with no positive tests, until the sudden discovery on New Year’s Eve (nay guisin!) in time to ban all the celebrations in open spaces - in that period at least 500,000 tests were conducted with not a single positive case. No-one thought this was odd or questioned if the tests were missing people, but of course there wasn’t actually any virus circulating in the community - but that’s not the point. I despair at the total inability of so many “scientists” to see the gorilla in the footy field.
I have finally found a copy of the Vaccine Choice Canada’s analysis of the PCR “test”. @PontiusPrimate , I’ve referred to this several times. It deals with Bayes’ Theorem as @Bob_sYourUncle has mentioned at least once.
As @Dimac has said, the absence of positives in 25,000 samples is impossible
The summary, using the manufacturers own specifications, you get 88% false positives and a 0.32% false negatives!
If you are short of time, watch from about 7 minutes. And don’t miss the 1 minute between 31:30 and 32:30!
I’m not saying anything except this. It’s people much smarter than me that say all the stuff I’ve repeated ad nauseam.
The PCR “test” is not a test. It’s a diagnostic tool that is being abused. I know nothing about the testing regime, controls (as highlighted above by @Bob_sYourUncle), or the cycles used.
But, that said, what I am saying is that in a police state (e.g. Victoria) lying about statistics would not be too surprising.
I know that wasn’t the point that you were making - it’s the point I’m making. I’ve seen a lot of data from the real world that indicates to me the problems of false positives for PCR is not a big issue. The Australian data is part of it. The Australia data is entirely consistent with a lot of other data that I’ve seen elsewhere in the world.
Just to clarify then, as I asked above - does it mean that anywhere in the world that we see a positivity rate of less than 1 per 25,000 PCR tests, you would say that is fraudulent?
Nothing is impossible PP - just so improbable as to be practically impossible. And if 25,000 without a positive is not enough for you, try 500,000! I haven’t looked at the stats, but every day since around November when the “second wave” finally petered out and there was a day of no positive cases, there have been between 15,000 and 30,000 tests done, until by NYE there had been 65 days without a positive case.
I’m not sure how much more it will take to persuade you that yes they did “lie”, and the thousands of scientists and experts who allowed this totally fraudulent deception to be passed off and proclaimed around the country also “lied” by keeping quiet. Did the labs put control positive samples in each batch? No-one ever asked. Did the labs find positive samples and retest them to find if they were false? No-one ever asked.
But not only that, nor the finding of virus in millions of litres of waste water from towns that didn’t have any cases, but back in ?September there were three cases in a town in Northern Victoria at a tyre shop visited by a positive-testing truck driver from Melbourne. This wasn’t revealed until almost two weeks after his visit, so a list of all the places the three had visited in that fortnight went out and a call for anyone there or with symptoms to get tested. Thousands queued up for hours to get the test, and totalled over 15,000 tests, but NOT ONE positive case was found, showing not only that the test didn’t find anything, but that the virus is so uncontagious other than by direct contact that only the people directly in contact with the known case were infected.
No-one noticed this, nor questioned the need to wear masks in public places or all the rest of the nonsense, and those who did got fined, like the pregnant woman whose house was busted for posting a notice on Facebook about an anti-lockdown rally. She has now been fined.
And yet that exact specificity for the PCR test is found all around the world, including in the UK, New Zealand, China, Taiwan, USA etc etc etc. Surely claiming it to be “improbable” is begging the question? Actually it might be normal. Clinging to theoretical arguments in the face of actual real world data is the same problem as mathematical modellers who get too attached to their model, when the data doesn’t support it but refuse to give up.
I’m still confused about this (as I indicated above). Do you believe that the authorities are falsely claiming that there are zero cases? Does that mean that you think there really are cases, and they are being hidden for some fraudulent purpose? That makes no sense to me - I must have misunderstood you. Why would the Australian authorities hide cases by falsely claiming zero cases, and the UK authorities simultaneously overstate cases to fan the flames of a “casedemic”. My logic circuits have fried…
I’ve not read that - but that is interesting. It reminds me of a study by a chap at Oxford who claimed to have found dead virus particles in the wastewater in Madrid from Summer 2019. I didn’t hear any more about that, so I’m not sure how accurate that turned out to be.
I’m not 100% surprised by this. I’ve been pointing out for months now that this virus doesn’t seem to spread uniformly, but rather makes abundant use of superspreaders. It’s one of the reasons that I think it is feasible to stamp out Covid, and one of the things that makes it different to 'flu.
Overall, I think that there is a lot discussion around false positive results from PCR that is just not that helpful. I used to think that could be a big issue, but as time has gone on I have changed my mind, and I no longer think that this is a big problem at all, for reasons that are becoming clear through this discussion, and for more that I am currently writing up.