“I think we should be told!” But obviously we’re not going to be, not until the awkward dissidents have finished digging out the truth piecemeal, a year or two after the covid panto has finally closed:
yes there is, @RhisiartGwilym . Many, many doctors and nurses have said so. All the statistics from every source have shown so.
It’s pretty clear really. This kind of refusal to look at the reality of the situation is understandable (it’s a horrible reality), but ultimately not useful for survival. It’s the same with those trying to avoid looking at the climate catastrophe, and instead finding all kinds of ways to try and deny that it’s happening.
It’s hard to look at, but pretending it isn’t there is not helpful.
Sorry P, but I have to stick with the ‘not proven’ stance, for now. I can quite imagine some hospitals in a hectic situation, but others - apparently - not. And there are too many dissenting voices saying this, plenty of them reputable professionals of appropriate expertise. You have to ask: WTF is going on!? The situation is simply not susceptible to magisterially-exact judgement. Not yet. O-MS rools!
Also, my lying memory, informed by my lying eyes, recalls two trips to Warwick hospital this month - supplemented by prompt new appointments scheduled for February, without cancellation or delay, where - unmistakably - the situation was normal, quite quiet, nothing hectic anywhere in evidence on the entire campus. Sure, one hospital does not a non-pandemic make. But my direct lying experience tallies with what the queriers are saying.
Something definitely isn’t right.
1 Like
Latest News – Lockdown Sceptics…
" It is also important to stress that this figure of 37,475 are patients admitted for any health reason, with a positive PCR test on admission or within the last 14 days – it is definitely not 37,000 patients who are unwell with Covid respiratory symptoms."
They are always “overwhelmed” at this time of year, and I’m sure that in the future of more hospital closures, cuts of beds and staff for the remaining beds, they will even more overwhelmed at any time of year.
Data on hospital admissions (‘with a positive PCR test’ as Bob points out) is collected and published, now daily I think: at Ourworldindata
https://github.com/owid/covid-19-data/tree/master/public/data; scroll down to
Download our complete COVID-19 dataset : [CSV] | [XLSX] | [JSON]
you get the whole covid spreadsheet. This includes columns on hospital admissions. Certainly according to this file, there are the amount of hospitalizations in the UK (GBR on the file, must have imported it from the Olympic committee, who are presumably having the rest of the year off  ) they say, and it’s much higher than in the spring last year.
) they say, and it’s much higher than in the spring last year.
I think it would be hard for this to be simply made up, with so many people involved at operational level and so many in the know. Also, is this happening in the other countries as well? It’s too big a conspiracy to contemplate IMO.
What’s wrong with the simpler ruses, which can be maintained at the level of politics, media and compliant health leaders? The fixation on ‘cases’, vaccines and the terribleness of Covid, except if you roll your sleeve up, and these pesky anti-vax terrorists as well. It’s a perfect narrative, who needs more?
2 Likes
Update: from Bobs Off-Guardian link:
"However, if we use this BBC article as a reference:
around 5,000 people were admitted to hospital with flu in the first week of January [in 2018]."
From the Ourworldindata file, the number of admissions with the positive PCR (used as covid hospitalizations) in the 1st week in January this year was 6193. So yes, indeed comparable.to that bad flu season; presumably worse in terms of deaths.
The BBC link says “Deaths from flu remained static with 27 in the past 7 days” (the link was from 11 January 2018). Deaths ‘with covid’ are far worse than that so if there is doubt it must be in that covid ‘diagnosis’ from just the PCR test, as most here will know was not supposed to be a proper use of the test, which was designed to confirm clinical suspicions arising from symptoms - ie to distinguish the illness, when there clearly is one, from other causes. So as ‘cases’ are not, as described, infections, with the number of cycles set unreasonably high it should mean that most ‘cases’ are fragments from previous exposures. This doesn’t get us very much further - as these deaths are still happening, and are a subset of the overcounted ‘cases’.
These could be the key questions in this line of thinking:
In what proportion of Covid hospital cases is Covid NOT the underlying cause of hospitalization?
in what proportion of Covid hospital cases was the Covid acquired IN the hospital?
Hi RG
I’m not sure why you discount the eyewitness testimony from so many doctors and nurses in the field, across many countries, in favour of a set of statistics that are far from clear. Especially when you are so sceptical of statistics in general. Can I remind you of Dr Kory:
“I run an ICU where there nothing but patients with covid. I don’t see any other disease anymore. All I see is covid, covid, covid, and they’re all dying… This is not the flu. I’m so tired of hearing that…”
Was he not telling the truth do you think? How about Dan at TLN? Lying? Together with loads and loads and loads of ICU testimony from the UK. I wonder why you ignore the clear clarion call from doctors and nurses on the ground in favour of vague hand-wavy stats based arguments?
I’ve been to Addenbrokes recently and they have completely re-arranged the hospital layout. Covid patients, admissions and wards are not accessible to the general public for obvious and very good reasons. I couldn’t take a picture of them if I wanted to.
It’s possible that Warwick has escaped the crush that is happening in other hospitals. What conclusions should we draw from that? Personally I go back to the clear fact that Covid doesn’t spread evenly through the country, but perhaps there is another reason why Warwick is so lucky.
Cheers
you say
Hmm… This is interesting, and I would be curious if there are any stats, or even a single example anywhere of a person being admitted to hospital who has a positive PCR test and is not suffering with Covid. If you could find such a thing I would, personally, be very interested. In the meantime I tend towards the old adage - “if it walks like a duck, looks like a duck and quacks like a duck, it’s probably a duck”. If someone is ill enough to be hospitalised and they are positive for Covid, then my first instinct is that they are struggling with Covid. Of course I could be wrong, and I am open to any evidence that anyone can dig up.
I am yet to be convinced that there are large numbers of false positives of covid. That doesn’t mean that it doesn’t happen, but simply that I have seen no evidence that this is big problem.
According to the office of national statistics the UK has not been this overwhelmed since 1940. This is in no way like business as usual.
Cheers
PP
Sure, there are some hospitals that are having a bad time. But I don’t believe we have a clear, overall picture yet of what the entire panoply is really like. We being the average plebs at home. And - in consonance with not trusting ANY stats - I don’t think we can quote figures and hope that they’re sound. Anecdotals from medical staff are always to be heard, as a priority. Plenty of those around. Clearly many of them are having a bloody awful time. But that doesn’t substitute for a whole-situation appraisal. We need both information sources. What a panoramic survey will tell us, once it gets done - with necessary hindsight - is anyone’s guess. I have no fixed position. I just don’t care to buy in, even slightly, to the obvious hype with which we’re being deluged right now. That stinks.
Hi RG
I hear the point your making.
Indeed. And this is what the function of the ONS is. They say - with data to back it up - that this is the worst time in the NHS excess mortality in the UK since 1940. A couple of anecdotes by folks wandering blindly around the wrong end of a hospital with a camera cannot disprove that.
If you want an overview, we should use the ONS. If you want on the ground reportage, use the people who are at the cliff face like the doctors and nurses I mentioned.
Random folks with cameras don’t add much as far as I can see.
I just watched a video today of some guy trying to take an older patient out of hospital. Taking the oxygen mask off the patient, arguing with the doctor and saying “no one has proved the existence of SARS-COV-2”, trying to make the doctor swap out antibiotics and steroids for vitamin C and vitamin D. The patients lungs were filled with clots because of covid. If the young man had his way, he would have killed that patient.
He filmed the whole thing on his phone to expose the covid scam. His testimony feels basically worthless to me. And many like him.
It’s time for all of us to face the harsh reality in which we’re living, or we’re not going to make it. This pandemic, the ones to come, and climate change that is raining down thunder on all of us, need to be taken seriously.
Sadly it isn’t. None of it. Not by our government, and not by those at the Off-G who are twisting themselves into ever tighter knots to avoid seeing what’s staring then in the face.
I have just posted this on another thread. UK Column on Wednesday did a short but very explicit piece on this, showing mainstream media headlines agreeing, except they were from 2019, 2018, 2017, 2016. So I guess even the doubters will be able to understand it.
1 Like
I find this almost unbelievable from an intelligent guy, and I assume it’s not sarcasm? I suggest you do two things to debunk (or reverse) your opinion. Vaccine Canada did an excellent analysis of the PCR “test” including using the test manufacturer’s own figures. When you’ve watched that, find out:
a) Who supplies the primers for the UK test
b) How many cycles are they using
If you still are not convinced, then we’ll have to agree to disagree.
Thanks @PatB I’ll take a look. So far I’ve seen lots of theoretical worries about false positive results, but zero examples in the real world. On the other hand I’ve seen several mass testing exercises that have shown zero positive results or very tiny numbers. How does one get zero positives out of 10 million tests if false positives are a really big thing?
If false positives were a serious real (as opposed to theoretical) problem then I would have expected more evidence of that in the mass testing that has been done…
As always, I’m very open to data showing otherwise. I’m always happy to consider that I might be dead wrong.
Cheers
PP
Hi, Pontius. I’m intrigued by your confidence in a PCR test. It has been criticised, not because it is a flawed test, but that it can be misused so readily by cycling the test sample multiple times to pick up even dead virus debris. This positive test is then used, politically, to use the measures that we are living under now. You don’t need to be on Twitter to read tweets, so I hope you will have a look at some of the criticisms of the PCR test (and some insight of Bayes Theorem too!) here…
Best wishes, Robert.
1 Like
Thanks Bob.
Yes, I get this and it is convincing in theory. In the real world data I’ve seen, there have been several examples of a population that gets a lot of tests (10 million at a time, for example) but produces zero or close to zero positive results…
If there were a lot of false positives we should never see that. There should always be a set number of positives, never zero. Similarly, the trends (upwards and downwards) of cases were pretty close to that of the ZOE covid symptom tracker (at least for the period when I was paying attention). ZOE had pretty good agreement with the ONS too, which uses PCR. That means that for all it’s problems, cases as measured by PCR agreed with cases as measured by self reporting symptoms through an app. Again, this should not happen if one measure (PCR) is horrible biased.
You go on to say
and I completely agree with that. This makes everything more complex because presumably this is something that can be dialled up or down depending what the political need is. That is politicians could direct labs to use more or less cycles depending what outcome they want.
I’m very willing to admit that this could be happening. Is it definitely happening? I don’t know.
Thanks for the links and tweets. Bayes’ theorem is definitely the correct way to think about this, but I’ll need a fresher head than I have right now to go through it 
Cheers
PP
Morning, Pontius, and everyone here too, of course!
A “fresher head” is a must to follow the Bayes Theorem, and indeed, why the difficulties of mass testing by laboratory tests done quickly and accurately is so very hard to achieve:
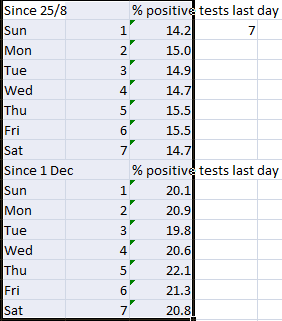
" Dr Craig: There’s a beautiful piece of evidence that’s just been produced by a physicist in Scotland called Christine Padgham, who is a force of nature and has gone carefully through all of the Scottish data. Public Health Scotland have been much more open with the data that they’re publishing, and they include in their publications the daily positive numbers, the daily negative numbers, the total number of tests done, and so you can actually get a percentage of positive tests per day that’s accurate. And when you look at the percentage of positive tests per day in Scotland, the percentage of positives is twice as high at the weekends than it is on a Monday. Now that cannot be anything to do with the disease.
That’s to do with the laboratories being under extraordinary pressures. It’s to do with people. The PCR testing, which is the test that we use for COVID, can be an incredibly specific test with a low false positive rate, but it can also be incredibly difficult to actually do because the first step is to translate your RNA to DNA and then you double the amount of DNA in the sample. You double it, and you double it, and you double it until you’re at a billion or a trillion times the amount you began with. What that means is that even the tiniest, tiniest amount of cross-contamination from other things in the lab can mean that you get the wrong result.
Whenever you run a test, you’re going to definitely put a certain positive in that test so you can make sure that the test worked properly. Every time they run a test, a positive control sample is being used. And if a little bit of RNA from that sample gets onto a glove, and gets onto the fridge door or something else around the lab, then every person that touches that fridge door is going to get contaminated, and the samples that they touch will get contaminated. The difference between a weekend and a Monday in a lab is that at the weekend you’re short-staffed, and people are tired, and the labs had all the problems that built up over the week hanging over. On a Monday, people come in fresh-faced. They’ve had a rest over the weekend, and the lab is thoroughly cleaned, and then you get out new chemicals that are all brand new and clean, and you start again."
“Follow” her, if you can, on Twitter, she is a star!
I appreciate the idea and the scepticism, definitely going to check out these two professionals-with-independently-functioning-brains.
What a nice idea - but is it true? I couldn’t get it to agree.
Those making the pcr test the standard have a lot to answer for. However pcr-positives will still include the real infections amongst the ones that aren’t real. I presume this will still be true irrespective of the possibility of contamination.
There are few false positives in the sense of the sars2 not being present at all - but there will be many that are false in the sense of the person not having a clinical infection.
‘They’ babble on about the number of ‘cases’ or ‘infections’ or ‘people who are infected’ when most probably are not. This has helped create a culture of ‘the Vaccine will save our normal lives’, and ‘HOW can I get the vaccine quicker’. etc.
A proportion of people get a positive PCR with a high Ct value and are obliged to self isolate because, not being told their Ct number, are not aware they are not actually infected or infectious.
The number of cases is open to external influence just by tweaking the number of Ct cycles. It may have been you Bob who posted (was it?) that the WHO were now advising bringing the Ct number down, and observing that this would reduce ‘cases’ timeously with the vaccine roll-out.
Pcr is fraught and should not be the sole driver of policy, I hope someone get to the bottom of it!
With you here RG - as here in CV-free OZ the hospital crisis is overwhelming us, along with endless talk of vaccines. I believe nothing I hear from mainstream media any more, if it conflicts with what I KNOW. And the one thing I do know, is that were HCQ+ to have been used generally, and still could be, then we would never have had this crisis of people ending up in hospital, nor the same spread of the virus, except perhaps amongst the old and sick.
Much more to say on this, when I have time. Every day in Australia there are at least 25,000 tests done, with NOT ONE positive case found. Doesn’t add up. And sometimes they expose themselves. Today it was announced that “fragments of virus have been found in waste water” in three country towns each 100 miles apart where there have never been more than one or two cases, so anyone living there or who has visited recently should get tested “if they have even the mildest of symptoms”. The reason they came up with this, after a fortnight without a single positive case, is because tonight the emergency state was due to lapse. It has now been renewed for another month. Case proven, they lied!
Thanks @Bob_sYourUncle - both posts with excellent content that I’ve now read. It inspired a lot of thoughts that I want to expand on, but it might not be today. I’ll follow up with you soon on the points you raise.
@Evvy_dense - some very good points there too. I think I’ll pick up my earlier thought about writing a more full post on some of my thoughts about PCR and false positives etc.
Cheers
PP
Exactly @Dimac - that is precisely the point I was making above. Zero false positives. I see that pattern all over the place, which makes me doubt the severity of the false positive problem in the real world. And I started off believing that it would be a real problem as we ramped up testing.
Turns out I was wrong
Cheers
PP