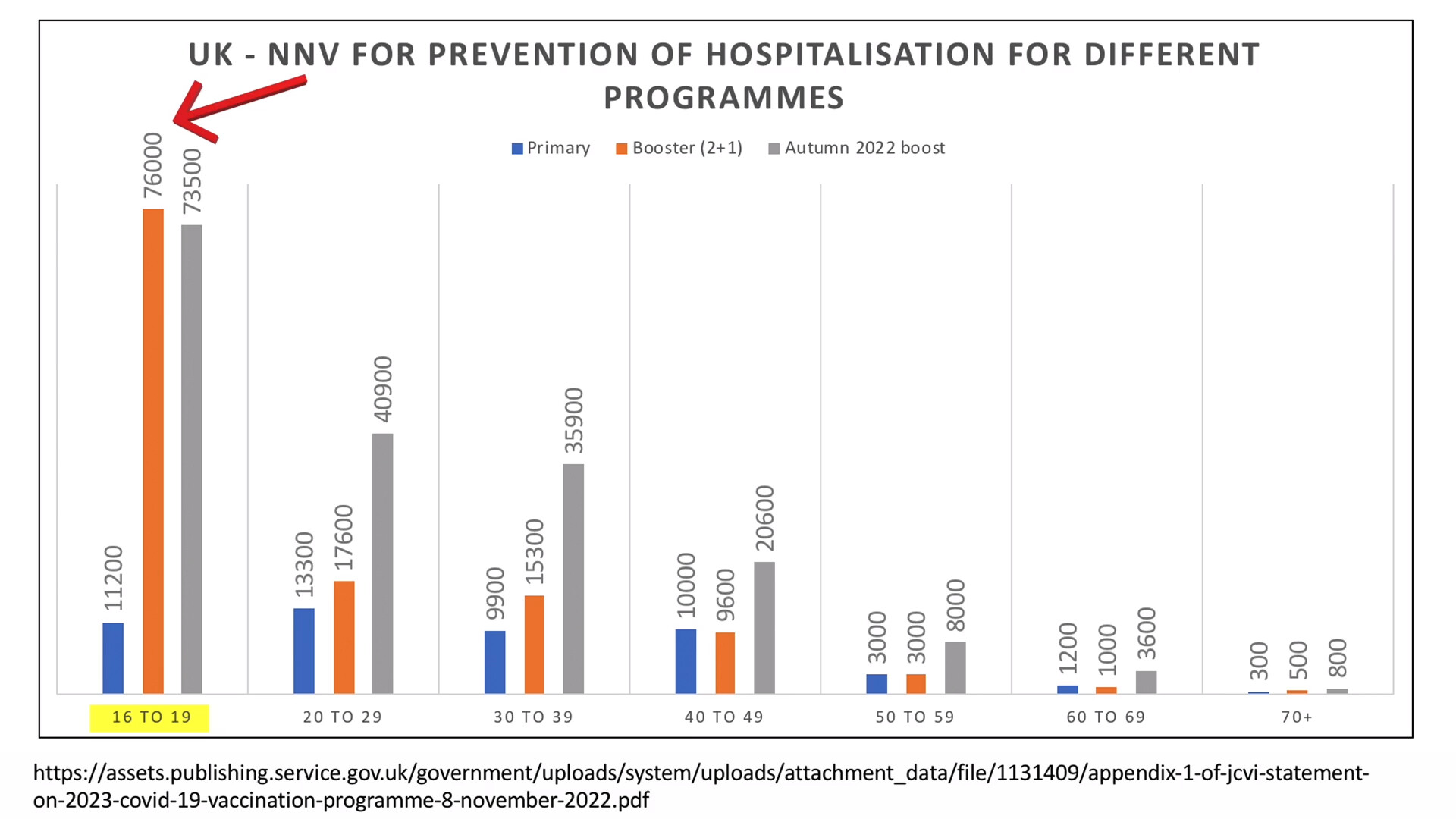
In summary, a new study shows "… mRNA vaccines were associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated … At the same time, from official UK stats, just look at the chart below.
One needs to ‘vaccinate’ (two shots plus booster, or should that be rooster?) 76,000 16 to 19 year-olds to prevent one hospitalisation. I’ll let you do the maths and yes, the study did not break it down by age groups, but you can draw your own conclusions.
Thanks PatB. One vs t’other - that’s about as succinct as it gets! One in 800 ‘saved’ from covid hosptalisation vs thousands of V’s needed to save another hospitalisation.
The serious adverse events reported are courtesy of the vaccine trials; it’s hard to imagine this doesn’t flatter the vaccines.
The claimed reduced covid hospitalisation ‘benefits’ are calculated on the basis of vaccine efficacy (Table 2 on the link). No numbers under the obligatory 50, naturally.
The more shots the less covid ‘benefit’ from the latest one.
This was from data ‘presented’ to the JCVI, so the data could be expected to be on its best behaviour.
How odd that the vaccination committee doesn’t need to consider serious adverse events
And there’s no consideration in this process of emerging cancer risks, or immune system weakening from repeated vaccine doses.
The c6000 number needed to vaccinate in my age group is plenty bad to be honest. And that involves rolling the dice three times.
Could the hospitalised include people admitted for non-Covid issues (broke their leg, etc) who then tested positive? If so I can imagine that getting an unvaxxed patient is a bit of a prize, and that extreme pressure is applied to ‘correct’ the situation.
I went for an ECG recently and the nurse said “I see from your notes that you haven’t had a flu jab”. I replied “That is probably correct as it never struck me as being necessary.”
“Okay well if you change your mind we have plenty…”
I didn’t vocalise my thought: “I’ll bet you have.”
Presumably, if I had reacted differently, she might have gone on to push for a covid jab too. A BoGoF kind of offer.
Seemed to be a fair few masked citizens in supermarket today, maybe one in ten.
Now it’s incredible official statistics from Canada - Alberta and BC.
A tale of two provinces - both with highly alarming data on excess deaths. Fortunately, the deaths could be blamed on other things - any port in a storm.
But less fortunately, vaccine booster data was showing equally alarming patterns.
Alberta ‘solved’ the political problem by…deleting the problem vaccine data. Excellent!
British Columbia, seemingly made of sterner stuff, boldly announced they would simply stop producing the bad data on vaccine outcomes - as it was becoming ‘hard to interpret’. As it would be, of course, if the obvious interpretation that is Not Permitted to be made, or even mentioned.
The problem was the data seems to relate the worsening outcomes directly to boosters.
I’ve not checked this in any detail - the graphs of this official data are at least clear (albeit yer last) and the story is capably told by Global Research; linking to (I presume) the original breakers Stew Peters and Mark Steyn of GB News.
You pays your money and you makes your choice…
ED
Alberta’s “Pandemic of the Triple vaccinated”: Excess Deaths Surge Past 10,000 — Evidence of Government Cover-up
Part III: As the triple vaccinated got sicker, govt deleted ALL vaccine outcome data…
Most people I know are ill, and this started last summer.
My cousin, who I think I mentioned in a previous thread, is now on her last legs. She has cancer of the bile duct. This is a rare and aggressive cancer. From diagnosis to death’s door has been about 3 months.
Hi @Evvy_dense, this report suggests the UK were well ahead of Canada in the data coverup process
“Vaccination status in cases, deaths and hospitalisations
Data on the vaccination status of COVID-19 cases, and deaths and hospitalisations with COVID-19, was previously published to help understand the implications of the pandemic to the NHS, for example understanding workloads in hospitals, and to help understand where to prioritise vaccination delivery.
From 1 April 2022, the UK Government ended provision of free universal COVID-19 testing for the general public in England, as set out in the plan for living with COVID-19. Such changes in testing policies affect the ability to robustly monitor COVID-19 cases by vaccination status, therefore, from the week 14 report onwards this section of the report will no longer be published. For further context and previous data, please see previous vaccine surveillance reports and our blog post.“
Thanks for the reminder CJ. I had a look back using the search facility on the forum. I found this from Jan 22
Just some rummaging on my part…
There is a link there to the latest (as of then) Vaccine surveillance report, which we discussed. I was looking to see if there was an announcement as to what exactly they said they were stopping producing - but I couldn’t find that.
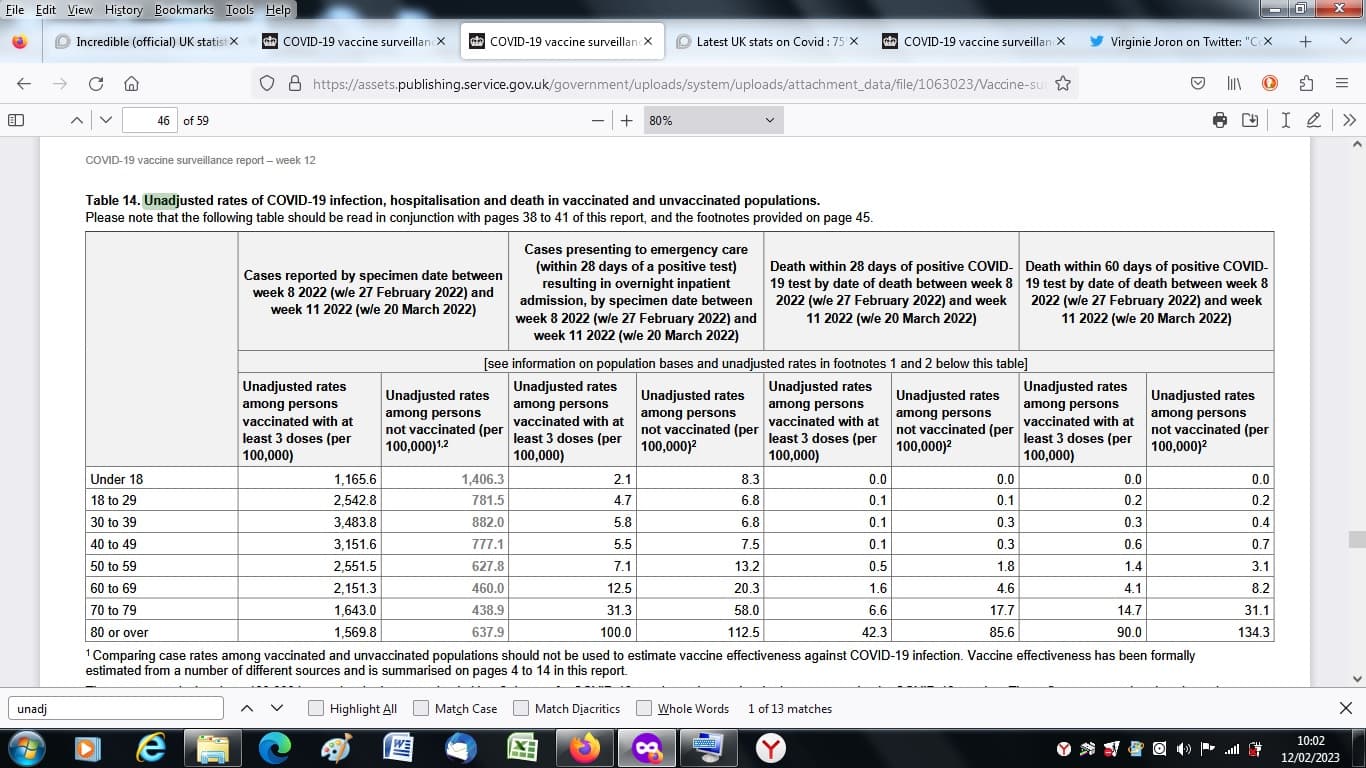
I think the thing they didn’t like was the greyed-out figure showing the unvaccinated got less covid, even pro-rata to their population.
The rest of the table seems to indicate a degree of vaccine effectiveness as far as serious illnesses are concerned; however as Norman Fenton pointed out they took liberties in specifying the unvaccinated population which led to it being severely underestimated. His team (I think it was them) suggested there was even no efficacy against covid.
The data here is likely to flatter the vaccine as it’s all 3 boosters shown. Boosters wane of course. This creates a time factor, with most of the people in this table (March 22) included likely to have been boostered relatively recently. The 60 day figure is conspicuously worse than the 28-day figure (which may include a lot of people very recently boostered). So that’s about 2/3 ‘efficacy’ (deaths after 28 days) gone down to 50% efficacy (deaths after 60 days). What would 120 days have looked like? And of course, other vaccine deaths and SAEs are nowhere to be seen.
But most people don’t read Norman Fenton, and the authorities would have been happy enough that the boosters could be portrayed as effective, if it wasn’t for the pesky greyed out figure - which strongly suggests that the vaccines were not only not reducing transmission, but increasing it. Even if covid was causing more deaths in the unvaccinated, the vaccine was making it worse by spreading the covid in the first place.
The per 100,000 population was arguably the only useful data they produced; even with the doubt about the size of the unvaxxed population, it would still show a trend, the worst thing is to chop and change. The excuse for not producing it any longer - due to reduced testing - is feeble as people must be being tested in the hospital in the first place to produce covid hosptial data.
Jumping to 2023 to see what is said now. You know there’s currents when you read things like this (from a week ago):
“As described above, several studies have provided evidence that vaccines provide some
protection against infection. Uninfected individuals cannot transmit. Therefore, the vaccines also
provide some protection against transmission.”
Oh dear. In lieu of population comparsions, we have the latest developments in bio-verbology…
COVID-19 vaccine surveillance report
Week 5
2 February 2023
" Vaccine effectiveness is estimated by comparing rates of disease (or positivity among those tested) in vaccinated individuals to rates in unvaccinated individuals."
Oh, good - is it?
Er, no.
It continues…
" Since very few individuals remained unvaccinated, VE of the fourth dose was
estimated as compared to those who had a waned third dose (25 to 39 weeks past receiving their third vaccine) (Table 2). "
The explanation continues merrily on, good luck making sense of it:
“The incremental VE for the fourth dose is therefore the level of protection that the fourth dose adds in addition to the remaining protection conferred by a third dose. These estimates, therefore, appear lower and are not directly comparable with estimates where VE is calculated relative to the unvaccinated. VE against hospitalisation was enhanced by a fourth dose; the incremental VE after 2 to 4 weeks was 58.8%. This waned to 10.8% at 20 or more weeks after receiving the fourth dose”
“All very clear, then - and don’t use this anyway!”
They then produce a table of ‘vaccine effectiveness’.
Even this gives a level of VE below 50% after 2 months.
The table which compared cases, hospitalisations and deaths per 100,000 population is no more.
Sorry bit of a jumble, probably lost the thread a bit
But yeah to answer your original point, the Brits were in there early, removing data on the ‘stitch in time’ basis ! Saves brazen manouvres later…
Here is their arse covering blog -a disinformation ( imo) blurb - on why we can only read the data in ways they lay down - but it doesn’t say anything about the deletion of the section in any update afaics :
“ Vaccination status in cases, deaths and hospitalisations”
because free testing had been ended!!
“From 1 April 2022, the UK Government ended provision of free universal COVID-19 testing for the general public in England, as set out in the plan for living with COVID-19. Such changes in testing policies affect the ability to robustly monitor COVID-19 cases by vaccination status, therefore, from the week 14 report onwards this section of the report will no longer be published.”
They ask us instead to look at other estimates and papers prepared by the usual suspects:
“ 1. UKHealthSecurityAgency,London,UnitedKingdom
2. NIHRHealthProtectionResearchUnitinVaccinesandImmunisation,London
School of Hygiene and Tropical Medicine, London, United Kingdom
3. NIHRHealthProtectionResearchUnitinRespiratoryInfections,Imperial
College London, United Kingdom”
and under “Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: funding from Public Health England for the submitted work;”
So to my mind effectiveness is being estimated by UKHSA or evidence of varying confidence is articled by UKHSA employees or PHE or by some with links to pharma and of course Imperial and SHTM - they also throw in a preprint for good measure!
The papers of course are written in medical opaquese ink, thereby allowing summaries to slide over the occasional half hidden caveat!
The whole data business is a dog’s breakfast afaics.
“We have previously found that using broader definitions of hospitalisation has given lower
vaccine effectiveness estimates, reflecting outcome misclassification where cases are likely
coincidentally positive whilst in hospital, without this being the primary reason for admission
(and therefore these cases cannot be prevented by vaccination). We, therefore, use stricter definitions to define a COVID-19 hospitalisation. Here, a COVID-19 hospitalisation is defined as requiring at least 2 days stay in the hospital and a respiratory code in the primary diagnostic
field. To estimate effectiveness against more severe disease we also estimate effectiveness for
those requiring oxygen, mechanical ventilation or ICU (Table 1).”
Or…We didn’t like the data on hospitalisations the way it was counted to scare the public in the first place, so for vaccine purposes we tightened it up.
What about deaths?
"Vaccine effectiveness against mortality with the Omicron variant (all sublineages using tests
taken until 5 September 2022) has been estimated for those aged 65 years and older using a
test-negative case control study design (all vaccines combined) (Table 4). "
I’m glad you reposted this link, I don’t know when they thought this one up.
‘Test negative’ design is a wheeze with previous form - in shoring up the flu vaccine. It is a way of conjuring up shortcut estimates for outcomes that you haven’t actually measured, using questionable assumptions that to me looked pretty optimistic, with the ‘science’ part not clearly in evidence.
Criticized here in this pre-covid article (my biased emphasis):
30/7/18 Measurement of Vaccine Direct Effects under the Test-Negative Design
Joseph A. Lewnard, Christine Tedijanto, Benjamin J. Cowling, Marc Lipsitch
" ABSTRACT. Test-negative designs are commonplace in assessments of influenza vaccination effectiveness, estimating this value from the exposure odds ratio (OR) of vaccination among individuals treated for acute respiratory illness who test positive for influenza virus infection. This approach is widely believed to recover the vaccine direct effect by correcting for differential healthcare-seeking behavior among vaccinated and unvaccinated persons. However, the relation of the measured OR to true vaccine effectiveness is poorly understood. We derive the OR under circumstances of real-world test-negative studies. The OR recovers the vaccine direct effect when two conditions are met: (1) individuals’ vaccination decisions are uncorrelated with exposure or susceptibility to the test-positive or test-negative conditions, and (2) vaccination confers “all-or-nothing” protection (whereby certain individuals have no protection while others are perfectly protected). Biased effect size estimates arise if either condition is unmet. Such bias may suggest misleading associations of vaccine effectiveness with time since vaccination or the force of infection of influenza. The test-negative design may also fail to correct for differential healthcare-seeking behavior among vaccinated and unvaccinated persons without stringent criteria for enrollment and testing. Our findings demonstrate a need to reassess how data from test-negative studies can inform policy decisions.
(From Full Text)…Recent years have seen growing enthusiasm about the integration of data from observational studies in decisions surrounding influenza vaccine policy (50), in part based on belief that vaccine direct effects— which have traditionally been measured in prospective, randomized controlled trials—can be recovered under the test-negative design (6,10,16,24).
However, uptake of the test-negative design by researchers and policymakers has preceded thorough examination of its theoretical justification (14). Our analysis highlights limitations to interpreting VE estimates based on the exposure OR from test-negative studies."
“Correcting’ for differential health-seeking behaviour!”
Really? It seems to be little more than an act of faith.
Tanks for highlighting the Conflicts of interest in statstics production.
I recall when they pulled data before they said vaccine efficacy would instead be shown by ‘modelling’.
On reflection, I agree with you the UK does a more masterly masking job. But at least a dogs breakfast would be objective…
WhatTF does this incredible gobbledgook even mean! Will even one in a thousand readers be able to get any sense of meaning from it at all, before giving up in disgust? I would accuse the authors of wilful intent to obscure, to cover their tracks and their arses, of course. Opaquese in-bloody-deed.
The more that comes out about this abominable covid scam the more utterly outrageous it becomes. See in particular the Latypova vid that I just posted: blatant criminality with intent.
Truly a time for widespread civil disorder leading to uprisings. Something extremely weird and obviously spectacularly criminal is happening across - at the very least - the Washington-subdued part of the world; which, thank heaven, is disintegrating as we watch, as the panicking gangsters in the Swamp, London and Brussels realise that the war they provoked in the Ukraine is blowing up in their faces, and is looking more and more likely to bring about defeat and destruction of the whole NATO gang at Russia’s hands. ‘Untergang/Downfall’ indeed; with the Rest of the World looking on, and drawing the unmistakable conclusions: liberation chances growing steadily!
The idea of a second Nurnberg Tribunal to try the criminals is looking more and more necessary - and likely!
Yeah I agree. Hard to understand and if they made it clearer something else would be clearer - the loadobollox.
Opaquese - good word, describes it. Royalties to @CJ1 .
Apologies, because I haven’t had time to read through all the links here.
Apparently, in the UK over the last year there’s been 60,000 extra deaths above the norm (even accounting for the covid bullshit, which was just rebranded flu).
It’s the same story for most other countries who forced their citizens to be injected with a bunch of shite.
A bunch of shite that came from totally immoral and corrupt pharma companies (who should all be in jail), a bunch of totally immoral and corrupt pharma companies who own all the politicians.