In keeping with the principle of starting a fight that you can win, ICAN have demanded that those with prior covid infection be afforded the same ‘freedoms’ as vaccinated individuals.
I say unanswerable, because CDC hasn’t been able to answer it, comprised as it is of 60 studies demonstrating the strength and duration of disease-acquired immunity versus its poor imitator.
It’s possible the CDC may be holding their fire for the court case ICAN threatens to bring, but all they could muster so far was a solitary and hardly relevant town study comparing vaxxed and unvaxxed immunity in people who had already had Covid-19.
Below is ICAN’s circular which updates on the situation.
ED
When the CDC chose to lift restrictions on the vaccinated, ICAN went to work. Through its attorneys, it formally demanded that the CDC also (at the least) lift restrictions on the naturally immune. It provided the CDC with over 60 studies reflecting that natural immunity is more durable and robust than vaccine immunity. The CDC’s response is shameful. It fails to address any of these studies, collectively involving millions of people, and instead cites a single irrelevant study of a few hundred people that does not even involve comparing vaccine versus natural immunity!
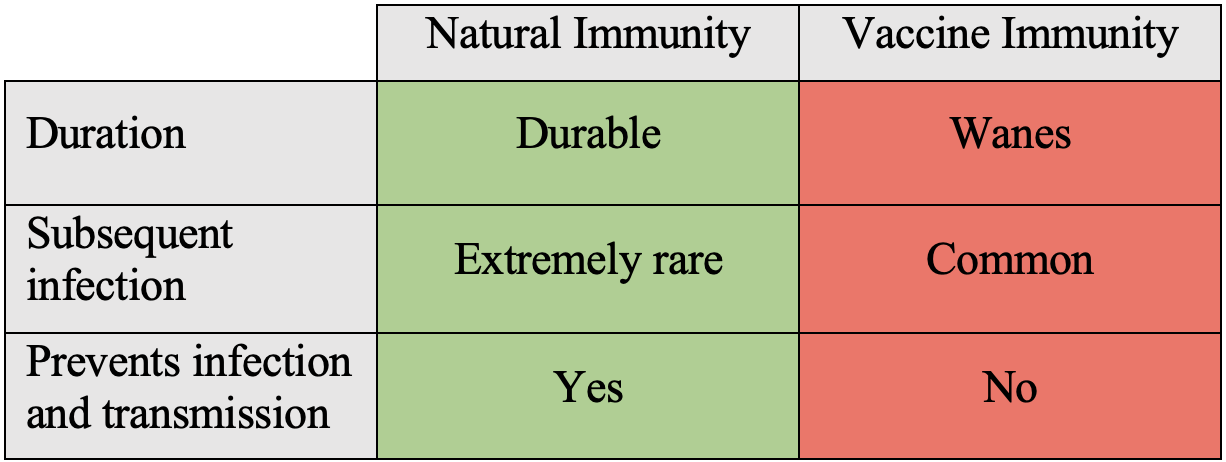
As reflected in ICAN’s formal exchange with the CDC, the available data and studies reflect as follows regarding the current virus causing most COVID-19 in the United States:
And here is the full story. In May, the CDC revised its recommendations for fully vaccinated people, lessening certain restrictions. This same guidance, however, made no mention of those who have already recovered from COVID-19.
Immediately after the CDC revised its recommendations, ICAN, through its attorneys, demanded that the CDC immediately include those who have recovered from COVID-19 in the same category as those fully vaccinated. ICAN’s demand was based on a robust body of science.
The CDC responded with a ridiculous form response thanking us for our “interest in” COVID-19. Our attorneys therefore submitted the letter as a formal petition to the CDC on July 6, 2021, to which the CDC is required by law to thoroughly respond.
In September, after even more studies had come out evidencing the robust and durable nature of natural immunity (and the waning efficacy of the vaccines), and having not yet received a response from the CDC (as they were busy cooking up the Kentucky study), our attorneys supplemented the Citizen Petition with 56 additional studies supporting that natural immunity is, in fact, superior to vaccine immunity.
Months after ICAN first contacted the CDC regarding natural immunity and submitted the petition, the CDC responded that it, “find[s] no basis to further modify the current CDC recommendation in this area until the science warrants it.” The CDC’s conclusion relied on one single study of Kentucky residents and ignored each of the 60+ studies ICAN submitted it the CDC!
ICAN’s attorneys have now submitted a reply to the CDC. In that reply, the attorneys explain that the Kentucky study, a retrospective study of only a few hundred people, is irrelevant as to whether it is appropriate for the CDC to lift restrictions on the naturally immune because the study did not compare naturally immune individuals with vaccinated individuals. Instead, it compared the naturally immune to the naturally immune with subsequent vaccination.
Even if vaccinating the naturally immune may improve immunity (which robust studies of millions of people show is not true, as detailed in our reply), it does not change the fact that natural immunity, alone, is better than vaccine immunity. Hence, if the CDC is going to lift restrictions on the vaccine immune, it is downright authoritarian to not do so for the naturally immune.
This letter exchange with the CDC represents the most comprehensive analysis of the current state of the science regarding natural versus vaccine immunity. We trust that you will not only appreciate reading and learning from this letter exchange with the CDC, but you will also enjoy it.
As for next steps, if the CDC does not, as it likes to put it, “follow the science” and lift restrictions on the naturally immune, we will be taking the CDC to court on this issue, that is federal court as well as the court of public opinion. And we look forward to doing so.
To share this legal update, please use this link: https://www.icandecide.org/ican_press/ican-eviscerates-cdc-in-formal-exchange-regarding-natural-immunity/