This is a monumental effort, from one of the leaders in repurposing drugs to treat Covid early.
I can’t help feeling Dr Kory (who is impeccably credentialled) imagined this letter would also be repurposed ![]()
Alternative title:
Widespread Evidence of Vaccine Harm, Waning or Negative Efficacy, and Early Treatment Still Works, Does It Not?
ED
Vaccine Exemption Letter For a 16 Year-Old Camp Counselor
[Part 1]
Parents have consulted me on the health risks and benefits of complying with summer camp vaccination mandates. Here is my letter documenting the informed consent discussion I held with one family.

Jun 7
June 6, 2022
Dear Tall Oaks Band Camp,
Grace Smith (not her real name ) is a 16 year-old girl whose parents have asked me to provide guidance regarding the health risks and benefits of complying with the Tall Oaks Band Camp mandate that all counselors be inoculated with the COVID-19 mRNA experimental gene therapy currently existing under Emergency Use Authorization in the United States. Although this medical intervention does not meet the traditional definition of a vaccine, the term vaccine will be employed for ease of use in the below.
I held a long informed consent discussion with Grace and her parents during which I provided the below data informing my recommendation. Note that the long-held (but now ignored) standard for informed consent requires that I fully disclose the most current and accurate data regarding all potential risks, benefits, and alternatives to COVID mRNA vaccination. Note that my interpretation of the below data was done consistent with the long-held (but pandemic-ignored) Federal regulatory standard that considers any adverse event or death reported in temporal association with receipt of a novel and/or experimental therapy to be caused by the intervention until proven otherwise . I recognize this practice departs from the recently adopted, ethically and morally troubling pandemic standard whereby U.S Federal and State Health Agencies’s dismiss adverse event reports as unrelated to the vaccines until proven otherwise.
Grace is a healthy teenager without significant past medical or surgical history. She is within normal weight and height for her age. Importantly, Grace has acquired natural immunity to COVID-19 given she tested positive in early March of 2022 after falling ill with fever, cough, sore throat and sinus congestion. Her symptoms began to improve by Day 4 from first symptoms, and by day 8 she felt fully well.
In the following, I will provide documentation of the informed consent discussion I held with them regarding a decision on whether to pursue COVID-19 mRNA vaccination. In the following, I solely relied on the most current, available data regarding;
1) risks associated with receipt of a COVID mRNA vaccination
2) efficacy of the COVID-19 mRNA vaccine in preventing illness
2) efficacy of the COVID-19 mRNA vaccine in preventing transmission
3) efficacy of the COVID-19 mRNA vaccine in preventing hospitalizations and death
4) efficacy of the COVID-19 mRNA vaccine compared to the protection offered by natural immunity
5) efficacy of the COVID-19 mRNA vaccine in the prevention of “long-haul” COVID
6) the risks of a healthy child suffering hospitalization and/or death from COVID
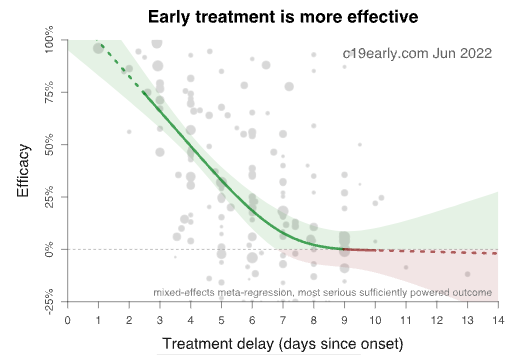
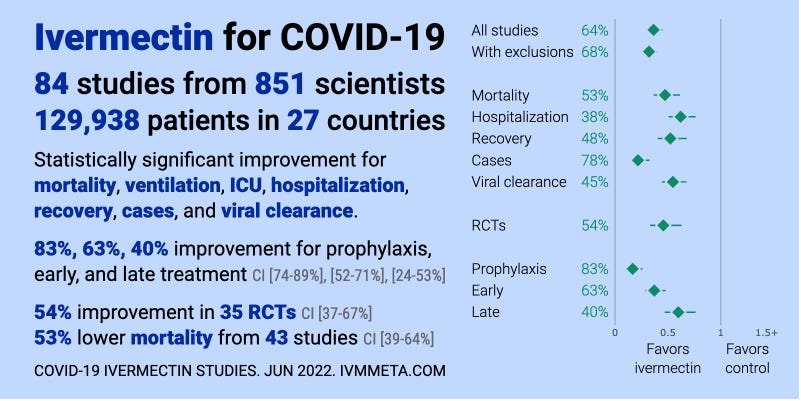
7) the efficacy and safety of alternatives to vaccination (i.e. reliance on effective early, anti-viral, and anti-inflammatory combination therapy)
As is standard in informed consent discussions, I first began with a review of the risks of COVID-19 mRNA vaccination.
1) RISKS ASSOCIATED WITH RECEIVING THE COVID mRNA VACCINE
Based on the below data compiled from peer-reviewed papers, Life Insurance Industry reports, and analyses of the Vaccine Adverse Event Reporting System (VAERS) database, it is my conclusion that a humanitarian catastrophe is occurring. This resulted from the rapid deployment of a raft of barely-tested mRNA vaccines in an illogical attempt to counter a fast-mutating coronavirus. I acknowledge that this assessment contradicts current “medical consensus,” which is that the vaccines are “safe and effective” and that vaccinating against a coronavirus is the dominant public health strategy across much of the world. There are a few reasons which may explain the discord between my personal recommendations and those of health agencies across numerous advanced health economies like the United States.
One is the dissymmetry between the data that I have painstakingly compiled and analyzed compared to the selective and near uniformly favorable data being disseminated across media, social media, and numerous high-impact scientific journals. One explanation for this discord can be found in recent FOIA-obtained evidence which revealed that $1 billion dollars was paid by the Department of Health and Human Services to U.S media companies to (blindly) support a media campaign to build public confidence in and uptake of COVID-19 mRNA vaccines.
A second contributing factor to the lack of scientific recognition of this catastrophe is that as of this writing, although over 1,650 case reports and small cases series of adverse events have been published in the medical literature, review papers reporting summary analyses of either the toxicity or poor real-world efficacy of the vaccines have been consistently rejected upon submission to medical journals, particularly high-impact ones. In addition to the rejecting of such studies, a number of journals have also illegitimately retracted papers that reported on the scale of adverse events despite those papers having successfully passed expert peer-review. The few published, peer-reviewed summary analyses that reported on either a lack of efficacy or on the excessive risks of the vaccines have generally appeared in lower impact journals that are systematically ignored by media outlets and academia. I chose to not only include, but to emphasize these important data sources as will be seen below.
In the setting of such widespread media, social media, and scientific journal propaganda/censorship of adverse vaccine data, the following information is unlikely to be known by the average citizen or physician in the United States. I invite any who want to challenge or validate my interpretations and conclusions to more deeply explore the underlying data sources using the hyperlinked references below.
Peer-Reviewed Literature
In this published paper analyzing data from the pivotal clinical trials used to support the novel mRNA vaccines (i.e. Moderna, Pfizer, and Janssen), Classen compared “all cause severe morbidity,” defined as “severe infections with COVID-19 and all other severe adverse events between the treatment arms and control arms respectively.” His analysis found a statically significant increase in all cause severe morbidity occurred in the vaccinated group compared to the placebo group.
In this paper by Walach et al, they calculated the Number Needed to Vaccinate (NNTV) to prevent one death from a large Israeli field study. They then accessed the Adverse Drug Reactions database of the Dutch National Register (Lareb) to extract the number of cases reporting severe side-effects and the number of cases reporting fatal side-effects.
- They found the NNTV to be between 200 and 700 to prevent one case of COVID-19 by Pfizer’s mRNA vaccine product.
- The NNTV to prevent one death was between 9,000 and 100,000 (95% confidence interval), with 16,000 as a point estimate (as you will see below, for younger healthy people, this estimate would tend to the higher end of a NNTV of 90,000-100,000 to prevent a single death).
- They calculated that for every 6 deaths prevented by vaccination, there were approximately 4 deaths reported associated with vaccination, yielding a potential risk/benefit ratio of 2:3 (note that deaths are consistently under-reported to such databases, thus a more accurate risk/benefit ratio for death would likely be inverted).
- They concluded that, “although causality between individual reports of adverse events and vaccination has not been established, these data indicate a lack of clear benefit, which should cause governments to rethink their vaccination policy”.
In this published paper by Jessica Rose, a world-expert analyst of the VAERS database, she found that, based on the ratio of expected severe adverse events to observed adverse events in VAERS for a number of conditions, the “underreporting factor (URF)” for COVID vaccine-associated deaths was 31. Using this URF for all VAERS-classified severe adverse events, as of October 2021, vaccines were associated with 205,809 deaths, 818,462 hospitalizations, 1,830,891 ER visits, 230,113 life-threatening events, 212,691 disabled and 7,998 birth defects."
This paper by Ronald Kostoff et al was retracted despite passing peer-review. However, in a personal review of the correspondence between the author and Journal Editor, neither I nor my colleagues were able to find a valid criticism of the underlying data analysis or conclusions. Therefore, I have incorporated this valuable study whereby they used a novel, best-case scenario, cost-benefit analysis which showed conservatively that there were five times the number of deaths attributable to each inoculation vs. those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreased drastically as age decreases, and the longer-term effects of the inoculations on lower age groups “may increase” their risk-benefit ratio (although this has not been demonstrated to date as can be seen below).
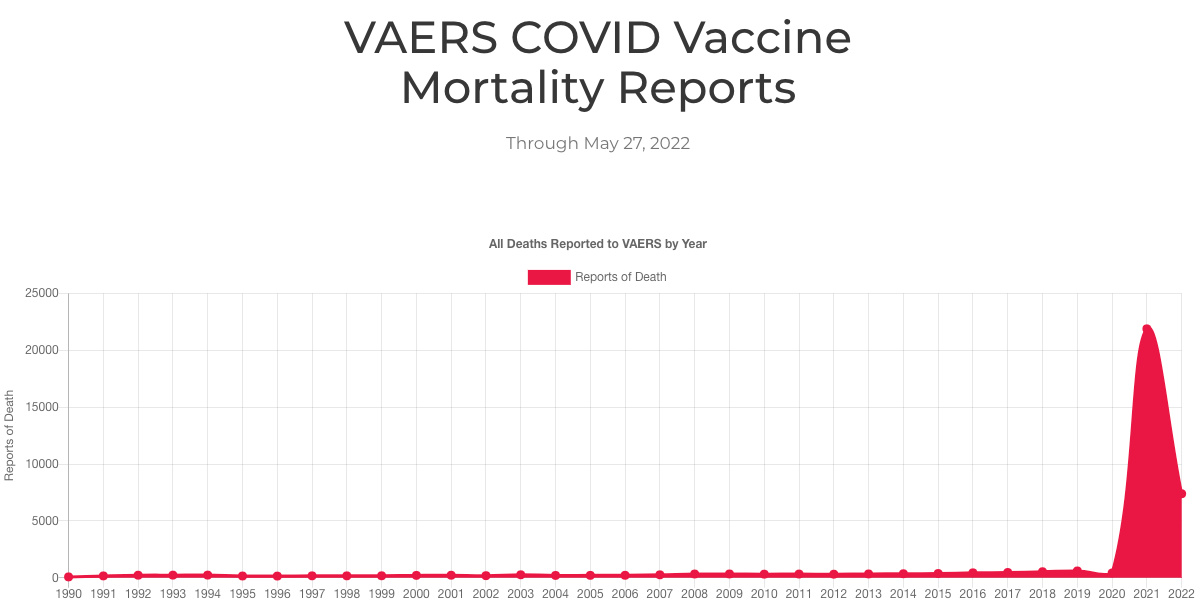
VAERS Data
As of April 22, 2022, in the United States alone 5,309 cases of myocarditis, 782,665 adverse events, 151,796 severe adverse events, and 14,613 deaths have been recorded in the Vaccine Adverse Event Reporting System following COVID-19 vaccination in the USA. It should be appreciated that the VAERS databases’s main limitation is that of underreporting, by a factor of at least 30-fold. The most concerning implication of under-reporting is in regards to the exponential increases in actual reports of death after vaccination in the past year compared to prior years of all vaccines combined.
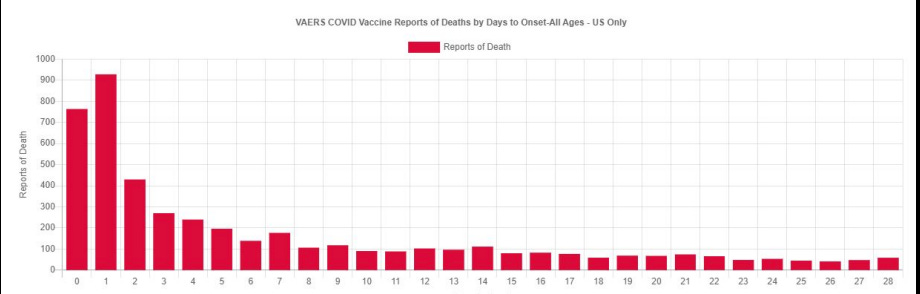
Even more damning is the temporal relationship of these reports to the date of the individual’s vaccination, which some authorities have attempted to dismiss as simply representing “background” deaths. The fact that the reporting of deaths decrease over time from date of vaccination (seen below), infers a worrying causal relationship whereas erroneously reported “background deaths” would instead appear in similar numbers each subsequent day after the date of vaccination.
Statisticians and analysts working with the Vaccine Safety Research Foundation (VSRF) have estimated the total number of deaths in the U.S caused by the COVID-19 vaccines based on the numbers reported to the U.S Vaccine Adverse Event Reporting System. In their white paper, they employed 9 different statistical prediction models and found that as of December of 2021, total deaths associated with the vaccines ranged from 148,000 to 216,000. Using the same methodology for the 14,613 COVID-19 vaccine associated deaths in the U.S reported as of May 16, 2022, the updated point estimate is approximately 599,000 deaths. The data and conclusions from these publications above provide support for identifying the vaccination campaign as the primary cause of the massive increases in Life Insurance claims among working-age Americans beginning in the second half of 2021, as will be detailed below.
Life Insurance Industry Data
Most concerning is a recent report of a large, unexplained rise in U.S life insurance claims amongst working age Americans of ages 18-64 beginning in early to mid-2021, timed with the vaccination campaign rollout. In a press conference, the CEO of One America, the $100 billion Life Insurance giant, publicly stated;
- “ what we saw just in third quarter, we’re seeing it continue into fourth quarter, is that death rates are up 40% over what they were pre-pandemic.”
- “deaths in this age group is 4 times higher than what would be seen in a “one-in-200-year catastrophe,” and that, “40% is just unheard of.”
- “every single other insurance company has also reported seeing the same – what’s most worrisome though, is that the biggest increase in excess deaths has come from traditionally healthier working-aged individuals under 65 – and not the elderly, who are the most susceptible to the Covid-19 virus.”
- “we are seeing, right now, the highest death rates we have seen in the history of this business – [and] not just at OneAmerica, the data is consistent across every player in that business.”
Financial analyst and former Blackrock Managing Director, Edward Dowd, reported similar historic increases in death claims over the same time period from discussions with major U.S life insurance industry executives; 57% for Lincoln National, 41% for Prudential, 32% for Hartford, 24% for MetLife and 21% for RGA.
In line with these data, a publicly available quarterly report by the Group Life Insurance Industry, covering roughly 90% of the employer-based policies, reported on Page 23 that younger age groups were suddenly dying at historically unprecedented rates beginning in Q3 of 2021.
The timing and magnitude of the historic rise in death and disability are also seen in German health insurance claims data and Medicare billing data.
Epidemiologic Data
An article published in the journal Nature reported:
- increases of over 25% in the number of ambulance calls in response to cardiac arrests (CA) and acute coronary syndromes (ACS or “heart attacks”) for young people people in the 16–39 age group during the COVID-19 vaccination rollout in Israel (January–May, 2021) compared with the same period of time in prior years (2019 and 2020).
- a robust and statistically significant association between the weekly CA and ACS call counts and the rates of 1st and 2nd vaccine doses administered to this age group. Note they found no observed statistically significant association between COVID-19 infection rates and the CA and ACS call counts .
- findings that aligned with previous studies showing that increases in overall CA incidence were not always associated with higher COVID-19 infections rates at a population level, and that the stability of hospitalization rates related to myocardial infarction throughout the initial COVID-19 wave compared to pre-pandemic baselines in Israel.
- findings that mirrored reports of increased emergency department visits with cardiovascular complaints during the vaccination rollout in Germany as well as increased EMS calls for cardiac incidents in Scotland.
In line with the above, as a result of a FOIA application in the state of Massachusetts, an analysis of the now publicly available death certificate data found that during 2020, the predominant cause of rises in all cause mortality were due to “respiratory causes ,” (i.e. excess mortality from COVID-19) while in 2021, the predominant causes were “cardiovascular .” The analyst concluded, “the official Massachusetts database of death certificates contains proof that C19 vaccines killed thousands of people in Massachusetts in 2021.”
Equally alarming are the massive rise in deaths among healthy, young professional athletes from around the world. Since the vaccination campaign was initiated, and as of June 4, 2022, there were approximately 1,090 athletes that suffered a cardiac arrest, with 715 of them dying as a result. The majority of arrests occurred in competition or training. The frequency of these events in comparison to historical data is highly concerning. In a 2009 review of professional athletes deaths, published in a prominent European Cardiology journal, they found that from 1966 to 2004, there was an average of only 29 sudden athlete deaths per year worldwide . Compare this number to just the month of January 2022 alone where 127 collapses and 87 deaths among professional athletes were reported. Overall, these athlete deaths reflect an approximately 22-fold increase in the year after the introduction of COVID vaccines, to date unexplained by other identifiable causes.
On March 10, attorney Matt Staver of Liberty Counsel presented data in court showing 127 VAERS-reported COVID vaccine-related deaths in the military in 2021. That is more than the 93 reported COVID deaths in the military since the beginning of the pandemic. Note that COVID deaths tend to be overestimated, while VAERS-reported deaths, especially in the military, are severely underreported.
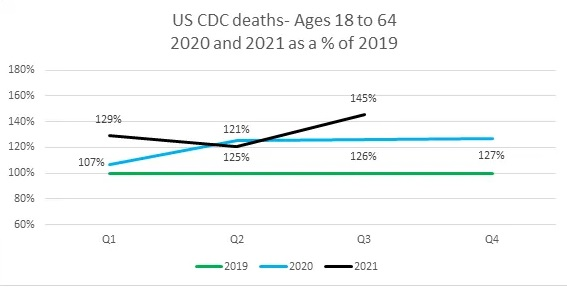
The CDC data provided in this article shows the timing of the start and the steady rise in all-cause mortality of working-age adults in the U.S, both overlapping with the start of the mass vaccination campaign. Although alternate causes of this historic rise in death have been considered, (i.e. COVID deaths, deaths of despair etc), the number of deaths from these causes is insufficient to explain the overall rise.
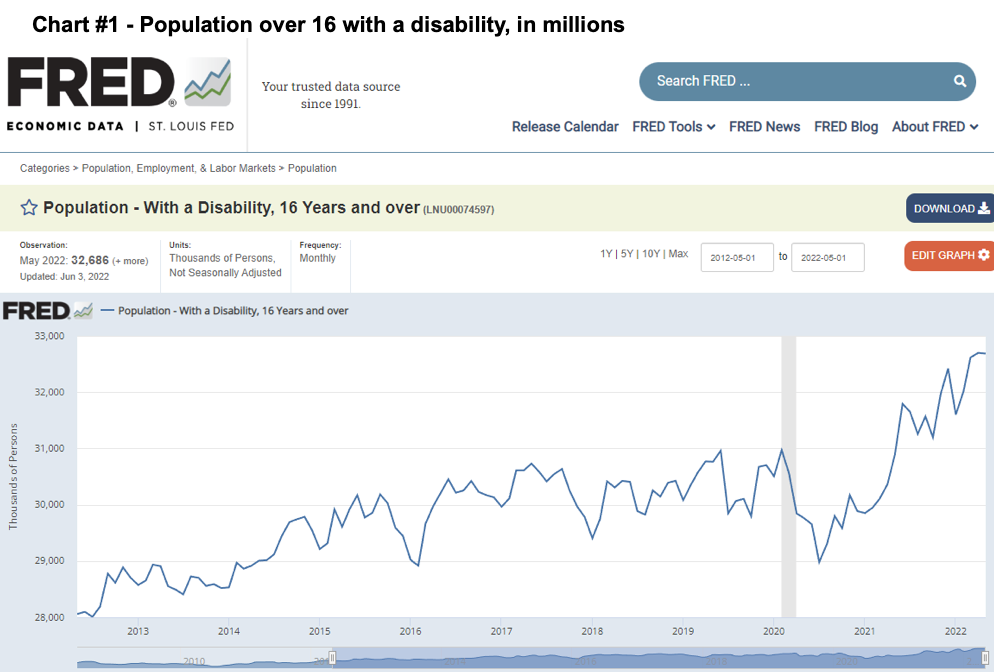
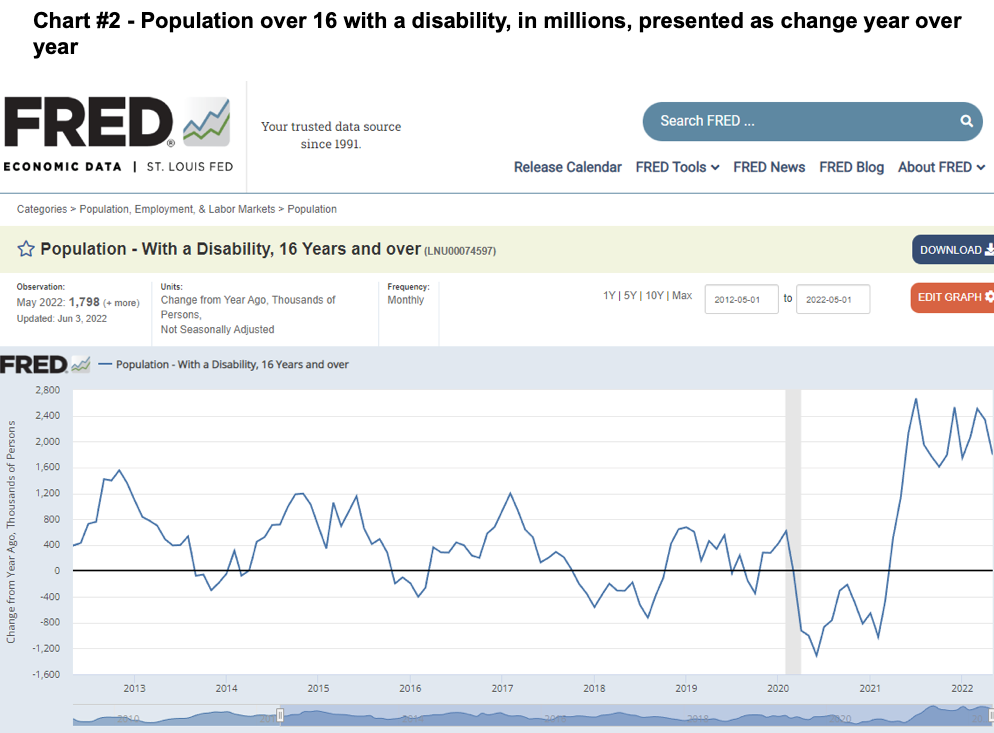
Rises in Disability
Associated with the massive rises in death claims are disability claims. The Bureau of Labor Statistics (BLS) surveys 60k households monthly to estimate the unemployment rate, and in this survey, asks households about disabilities as well. From the BLS data, for Americans over the age of 16:
-
After declining in 2020 (and stable for five years prior), in Dec 2020 there were 29.9 million Americans disabled. This is a disability rate of 11.4%.
-
At year end 2021, there were 32.4 million Americans disabled. This is an increase of 2.5 million people and a disability rate of 12.4%. This is a record number and record percentage rate.
-
As of May 2022 there were 32.7 millionAmericans disabled. This is an increase of 2.9 million people since Dec 2020, the start of mass vaccinations. This is again a record number and percentage rate.








{kind=link}