85m video.
https://articles.mercola.com/sites/articles/archive/2021/09/07/long-term-covid-vaccine-dangers.aspx
It’s pretty technical.
A transcript is below. I’m not sure if the video will disappear in 48 hours due to the embargo on Dr Mercola’s output.
I still found it worth listening to/watching the explanations made in the flesh, it dispels the idea that these are just some kinds of mad rants, as these are obviously experts talking technical. Criticism of Mikowits tends to be a long way below the level of her evident level of expertise, in an effort to distract people from taking her seriously - rather than engaging technically with what she is saying.
ED
Story at-a-glance
*mRNA-based COVID shots have used codon optimization to improve protein production. A codon consists of three nucleotides, and nucleotides are the building blocks of DNA. Use of codon optimization virtually guarantees unexpected results
*Replacing rare codons must be done judiciously, as rarer codons can have slower translation rates and a slowed-down rate is actually necessary to prevent protein misfolding.
*Stop codons, when present at the end of an mRNA coding sequence, signals the termination of protein synthesis. According to a recent paper, both Pfizer and Moderna selected suboptimal stop codons
*The COVID shots induce spike protein at levels unheard of in nature, and the spike protein is the toxic part of the virus responsible for the most unique effects of the virus, such as the blood clotting disorders, neurological problems and heart damage. To expect the COVID shot to not produce these kinds of effects would be rather naïve
*Other significant threats include immune dysfunction and the flare-up of latent viral infections such as herpes and shingles. Coinfections, in turn, could accelerate other diseases. Herpes viruses, for example, have been implicated as a cause of both AIDS and chronic fatigue syndrome
THE TRANSCRIPT
Possible Adverse Biological Reactions From COVID-19
Vaccinations:
A Special Interview With Judy Mikovits, Ph.D., and
Stephanie Seneff, Ph.D.,
By Dr. Joseph Mercola
Dr. Joseph Mercola:
Welcome, everyone. Dr. Mercola, helping you take control of your health. And today we’ve been
able to put together the dream team when it comes to the coronavirus vaccine. So last week I
interviewed Dr. Stephanie Seneff and it was a really well-received expansion of the paper she
wrote, probably the finest paper on exposing what the vaccine is doing. And we had nearly
500,000 views. And this week we’re going to double that with Judy Mikovits joining us. This is
her third time I believe we’re connecting and she’s going to help us put all the pieces together and
refine and expand on this devastating issue with the vaccine. I can’t believe it’s been almost a
year since we last connected, but in that interview, you discussed specifically the concern about
these vaccines that were going to really dramatically affect fertility rates through this spike
protein-generated antibodies to the syncytium. And we’re seeing that.
Judy Mikovits:
Yeah.
Dr. Joseph Mercola:
We’re not only seeing that; we have the CDC (Centers for Disease Control and Prevention)
literally, weeks ago, recommending pregnant women get the vaccine, and then they decrease the
age down to 12 to 15, the kids get this vaccine. So it’s just crazy. Well, welcome everyone, and
thank you all for joining us. So maybe you can respond to that right off the bat because to me
this whole issue with the vaccine, the whole pandemic seems to be targeted towards essentially
giving everyone the vaccine. And you can support this assertion because anything that disputed
the vaccine was censored and disengaged. Even drugs, drugs like ivermectin,
hydroxychloroquine. Not even just natural nutrients. They forced me with personal threats to
take all the information about nutrients and COVID vaccine off my site. So this is leading the
way to have everyone get the vaccine. We’ve got almost a quarter of a billion doses of vaccines
have been administered in the United States. As we recorded this, by the time this is viewed,
we’re nearly 5,000 deaths from the vaccine, 5,000 deaths. There are so many more statistics
going but Judy, let’s start with you. It’s been a while. We just talked to Dr. Seneff last week and
what’s your latest take on what’s going on because we’re really interested in it.
Judy Mikovits:
Well, I guess our latest take on what’s going on is exactly what we expected or unfortunately
anticipated at the molecular level because the spike protein causes the disease. The SARS COV-
2 infection never was what they said it was. There was no infection asymptomatically. It’s a
monkey virus coming out of a monkey cell line and that’s the problem, but the spike protein is
clearly the disease. So you just injected the envelope of HIV (human immunodeficiency virus),
XMRV (xenotropic murine leukemia virus–related virus) if you will, syncytin gammaretrovirus
envelope, and SARS ACE2 receptor binding domain. That’s not a vaccine as we’ve been saying.
It is the disease-causing agent. It’s a bioweapon. So now your cells are all producing that
bioweapon and you’re going to take out the innate immunity and NK cells and dendritic cells as
we know with the HIV and the syncytin domains. You’re going to disrupt your white blood cells,
your immune response. You’re going to turn on anti-inflammatory cytokine signature in every
cell of the body and exhaust your natural killer cells’ ability to determine infected cells. It’s the
nightmare we predicted.
Dr. Joseph Mercola:
Yeah. So have you had a chance to read Stephanie’s paper?
Judy Mikovits:
No, I haven’t.
Dr. Joseph Mercola:
All right. Well, we can go over that in detail but-
Judy Mikovits:
That would be fun since I tried to, but I thought it would be fun.
Dr. Joseph Mercola:
It’s definitely an incredible paper. It’s like 40 pages.
Judy Mikovits:
Well, I thought it’d be fun to see what I think without knowing.
Stephanie Seneff:
Learn it from me.
Dr. Joseph Mercola:
It took me two days to read.
Judy Mikovits:
I am going to open it up right now.
Dr. Joseph Mercola:
One of the things that she exposed and it was just fascinating is that this spike protein that they’re
causing our body to produce, if you indeed received the vaccine, is that this spike protein is not
the same spike protein that the SARS COV-2 virus has. It’s completely genetically engineered.
They substituted the nucleotides in the messenger RNA for methyl-polyuridine instead of just
uridine or uracil.
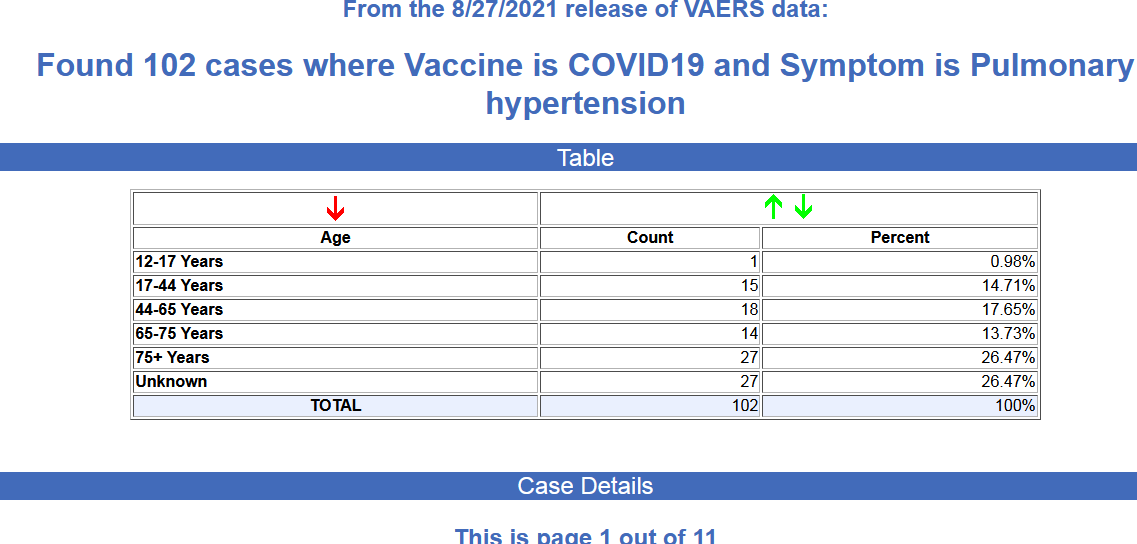
protein from getting in, which means the protein and my guessing, it’ll just stick there on the
ACE2 receptor disabling it. And when you disable ACE2 receptors in the heart, you get heart
failure. When you disable them in the lungs you get pulmonary hypertension. When you do it in
the brain you get stroke. I mean, there are lots of nasty things that happen from disabling ACE2
receptors. So their body’s going to be producing all these spike proteins in the spleen and then
shipping them out and then they’re going to get into the circulation and cause lots and lots of
trouble, I would predict. And I don’t know if Judy would agree with that.
Dr. Joseph Mercola:
Well, let me just insert something here before she responds and that these are shipped out in
particle sizes that are between 20 and 40 nanometers, these exosomes, and they easily penetrate
the cell membranes at that size. One more question for you, Stephanie. It just occurred to me, is
the messenger RNA that’s obviously been genetically altered to help produce the spike protein,
the code that it’s designed to produce, is that for the spike protein with the extra prolines that
keep the protein open when it’s attached to the receptor?
Stephanie Seneff:
Yeah. It’s in the RNA code. And the other thing they’ve done with the RNA is they’ve stuck in a
lot of extra Gs and Cs, which makes it much better able to make proteins. So they’ve redesigned
the actual RNA of the virus in many ways. We mentioned the methyl-pseudouridines, but also
everywhere they can, they’re putting a G or C, and GC-enriched RNA is much better at making
proteins. So it’s turned up the game on the natural virus by a thousandfold, making the RNA
much more willing to make a protein. So it’ll make a lot more spike protein than you would’ve
had from a natural RNA virus.
Dr. Joseph Mercola:
Okay. Yeah. So, Judy, with that information, this has got to be almost exponentially worse than
you initially predicted a year ago. So maybe we can have your comments on it now.
Judy Mikovits:
Well, yeah, exactly with that information, it makes it exponentially worse because all we’re
thinking is that, okay, one, the serious problem is that lipid nanoparticle as we said, but we’ve
seen that in Gardasil and some of the newer hepatitis B vaccines, we’ve seen similar of those
lipid nanoparticles. So we’ve got an idea of how to break those down, but when the RNA as
Stephanie said, is not the RNA of a natural virus, they remove cleavage sites so it breaks down.
And then you’ve got RNA as a danger signal expressing those GC-rich areas can look like
patterns of bacteria and virus at the same time. So we use poly(I:C) [polyinosinic:polycytidylic
acid]to signal the cell to turn on the type I interferon pathway. And because this is an unnatural
synthetic envelope and you’re not seeing poly(I:C), you’re not getting the type I interferon
pathway, that you’ve bypassed the plasmacytoid dendritic cell, which combined with IL-10
talking to the regulatory B cells decides what subclasses of antibodies to put out.
Judy Mikovits:
So you’ve bypassed the communication between the innate and adaptive immune response so
you’ve missed the signaling of the endocannabinoid receptors with those lipid nanoparticles
being 30 to 50 nanomolars is about half to a third the size of the natural viral particle. And this is
how we always determine the difference between exosomes and viruses because viruses are
about 100 nanomolars. You still can’t filter them away from it easily.
Dr. Joseph Mercola:
Is it nanometers, not nanomolar?
Judy Mikovits:
Yeah. Sorry, nanometers. Yeah, nanometers. So the size of the virus is like one-third of the
normal virus. So this is how on an electron micrograph we distinguish exosomes, extracellular
vesicles. It’s not that they’re not there and the diseases and interestingly, they carry these
defective messages. That’s one of a large part of Dr. [Francis] Ruscetti and my work over the last
30 years is to say you don’t need an infectious transmissible virus, these defective viruses all the
way through HIV and everything we’re seeing, just pieces and parts of these viruses are worse as
Stephanie is saying because they also turn on danger signals. They act like danger signals and
pathogen-associated molecular patterns. So it synergistically just leaves that inflammatory
cytokine signature on that spins out of control your innate immune response. It just cannot keep
up with the myelopoiesis. So you see a skew away from the mesenchymal stem cell towards a
TGF-beta regulated hematopoietic stem cells. So you could see the bleeding disorders on both
ends. You can’t make enough firetrucks to send to the fire, whether it be eosinophils, all your
innate immune response can’t get there, macrophage subsets, so can’t do it. And then you’ve just
got a total train wreck of your immune system.
Dr. Joseph Mercola:
Yeah.
Stephanie Seneff:
This makes so much sense. And in fact, I’m really excited to hear Judy talk about some of this
stuff because I was just reading over the weekend about this type I interferon, which I think is
actually very, very interesting with respect to these vaccines because we are seeing several
different kinds of evidence of herpes and varicella infection, shingles, people getting shingles
right after the vaccine or getting herpes or getting a cold sore, herpes flare-ups. So basically
you’ve got these latent viruses that are not bothering you at all until your immune system gets
completely distracted by this crazy thing going on in the spleen with all this messenger RNA and
all these spike proteins. The immune cells are distracted from their other job of keeping these
viruses in check. And so you get these other conditions showing up and there are several. Facial
palsy, for example, Bell’s palsy, there are like over 1,200 cases of Bell’s palsy reported after the
vaccine in the Vaccine Adverse Event Reporting System. And Bell’s palsy, when you look at the
research of what causes that, they really point to the herpes virus and the varicella virus as being
the source of Bell’s palsy. So what you’re seeing I think is a suppression of that. And I’d like to
hear Judy’s take on that. And type I interferon system is what you need to keep these guys in
check.
Stephanie Seneff:
And so those viruses are getting enabled and they’re causing symptoms. And then that is actually
a very bad sign. I’ve looked over the weekend, I looked at a lot of data to see that if a woman
who’s pregnant has a herpes flare-up during pregnancy, she has a twofold increased risk of
producing an autistic son. And also people who have Parkinson’s disease, they had a study on
200 Parkinson’s patients compared to 200 age-matched, gender-matched controls, six of those
Parkinson’s patients had at least one episode of Bell’s palsy in the past, whereas none of the
controls had. So it looks to me like the Bell’s palsy is an indicator of a future risk of Parkinson’s
disease. And if you get a herpes flare-up in pregnancy, and of course, they’ve done experiments
with mice, they know they can cause the offspring of a pregnant mouse to become autistic just by
giving immune flare-up.
Stephanie Seneff:
And it’s a well-known way to produce autism in the offspring is to have an acute immune
response by the mother mouse during pregnancy. So I think we’re asking these pregnant women
to go get this vaccine, not only have the potential to abort the baby, potentially not being able to
have another child after that is a real possibility, I think, or to end up with a child with autism or
maybe some other kinds of problems because of that intense immune flare-up during pregnancy,
which is a very dangerous thing for the baby, I think.
Dr. Joseph Mercola:
Yeah. So there’s not much better person to address this than Judy because interferon, as I
understand from reading your most recent book, is the catalyst for her going into science once
you saw it discussed in the front cover of Time Magazine. And she addressed a big portion of her
initial scientific career studying it. So why don’t you take it from here, Judy?
Judy Mikovits:
Yeah, exactly. Type I interferon and it’s interesting because we’re always talking about type I
versus type II responses. And unfortunately in the field, the language the clinicians call type I
and type II are very different things than the research immunologist people because of course
type I is not the innate immune interferon. Type I responses are adaptive and the gamma
interferon. So the innate immune interferon is your whole frontline. And we know from my
initial work, remember AIDS patients, people who got AIDS from HIV had a dysregulated type
I. So they could make gamma interferon, rather it was skewed towards TH-2, IL-4, IL-5, towards
parasites, worms, helminths. That’s a type II response and isn’t it curious that we have that
ivermectin and anti-parasitics work.
Judy Mikovits:
There’s a paper that I used and probably have used it, Dr. Mercola, in all of our talks and I know
Stephanie and I usually put it on the screen, it has to do directly with what she’s saying again
about another family of viruses, the herpes viruses. And the paper’s called “War and Peace
Among the Microbes.” So what we always saw in AIDS patients, and this was the age-old
argument of “Is it herpes viruses causing AIDS, HHV-6 causing ME/CFS?” that were long
associated. And it’s not until the virus families partner up, the retroviruses take out the type I
interferon pathway as does Borrelia as they dysregulate the plasmacytoid dendritic cell. Then the
HIV sequences do most of their damage to the monocyte, macrophage, where Stephanie just said
it’s kept latent. So she mentioned GC-rich regions in the sequences. Those regulate DNA
methylation pathways, which then silence the virus.
Judy Mikovits:
So at multiple levels, you cut out your frontline troops, you direct the responses, as Stephanie
said in the beginning, directly to the spleen, send everybody to the spleen for the explosion, but
you bypassed the mucosal surfaces and the resident stem cell monocyte, macrophage. So every
single tissue like alveolar macrophages in the lung, Kupffer cells in the liver, that was my Ph.D.
thesis, is if you kept the viruses latent then they don’t stimulate those cascades, which can be
organ system-specific. And this is what we saw caused AIDS. HIV did not cause AIDS. You
needed more than one pathogen to take out natural killer cells in the case of Borrelia. And then
think about mycotoxins and the part, so you’re damaging, you’re synergizing the ability to
dysregulate the innate and the adaptive, and then you dysregulate the activation of your
endogenous viruses, your endogenous syncytin, and your gammaretrovirus envelope is
expressed.
Judy Mikovits:
You’re seeing synthetic or non-self or in the back. And then again, you’re seeing the sequences
from activating the latent viruses like herpes viruses, which are also in part regulated by DNA
methylation. So they tether to the inside against the nuclear membrane. So you’ve got herpes
virus coinfected cells with HIV or retrovirus because you’ve got your gp120 sequences on the
spike protein in these sequences. And you’ve got the XMRV gammaretrovirus sequences, which
are syncytin. So syncytin is like Velcro, so anywhere syncytin is around, you’re sticking cells
together so that causes inflammatory responses. You break down, sorry, the megacarrier sites. So
you break down your platelet responses. It’s just an explosion of a nightmare of crippling every
area of your immune response.
Dr. Joseph Mercola:
Yeah. So just to backtrack a bit for those who may have not watched your earlier interviews
where we discussed this, but the SARS Cov-2 spike protein that we’re talking about very clearly
now has been shown to be engineered. This is not something that spontaneously mutated. And
it’s evidenced by the fact that you have this HIV protein integrated into that. So can you confirm
that and give more details on it? And did you also say the XMRV protein is within that?
Judy Mikovits:
Yeah, because the gammaretrovirus, our endogenous gammaretrovirus is called HERV-W
(human endogenous retrovirus type W). And HERV-W is all the way back in genesis in our
original endogenous genome. So HERV-W expresses only Human Endogenous Retrovirus-W,
it’s the gammaretrovirus that expresses only the envelope. That envelope protein is called
syncytin because in retrovirus envelopes the envelope alone is enough to cause the disease.
They’re calling it the spike protein, just to throw us all off. And as we know, if you culture it
using the Baric-Shi Zhengli “no-see-um” method, what did we do? We introduced a mutation
into an infectious molecular clone. We grew it in a cell line, Vero E6 monkey tissues that have
SIV and other gammaretroviruses because those are the cell lines we’ve been using in Fort
Detrick and Wuhan since the mid-1990s mixed with a lot of [inaudible 00:23:29] tissues.
Judy Mikovits:
So when you introduce a faster-growing strain and virus into the cell line, it’s called “no-see-um”
because as it replicates really fast without editing functions, the virus can’t go back and fix the
mistakes like our DNA polymerase does. So it goes right through it, makes mistakes and you
have a recombinant in every fermentation process. So the spike proteins then in a method you
can’t detect, you’re going to change the expression of the protein. So syncytin is the
gammaretrovirus, it cross-reacts with the mouse and monkey gammaretroviruses. Monkeys,
mice, all have syncytin. And then so your endogenous viruses express especially during
hormonal cycles. And when it’s expressed in the wrong place, like in the brain and the spinal
cord, it’s long been associated with the inflammatory disease and the destruction of the myelin
sheet in multiple sclerosis.
Judy Mikovits:
So syncytin expressed in the wrong place gives you the multiple sclerosis diseases, the paralytics
diseases. We know, as Stephanie just said, Parkinson’s associated with type I interferon
responses. Kent Heckenlively wrote a book with Joe Cummins about type I interferon. We’ve
dug into it a lot more in “Ending Plague,” hopefully, our last book. We’re now starting to
appreciate really that there is a low-level expression of our endogenous virome all the time and
that in our innate immune response it’s trying to shape and educate our type I interferon
pathways. And at least there are alpha, beta one, two, three. There are a lot of type I interferons
that really fine-tune the innate immune response to keep the flame, I say the dimmer switch, on.
Inflammation is now at the heart of all of these diseases.
Judy Mikovits:
So it’s absolutely fascinating, and the final problem that is the biggest problem is these exosomes
because as we’ve mentioned, your body’s exosomes are like your cells’ response to express its
regulatory RNAs, small inhibitory RNAs, long-chain non-coding RNAs, which Dr. Ritchie
Shoemaker has long associated with people with chronic Lyme and ME/CFS and the TGF-beta I
pathway. Remember I just said, TGF-beta 1, that’s the master switch to turn on which type I,
which myelopoiesis. We see cancers younger and younger accelerated so it’s just accelerated
death. But these exosomes are packaging not only RNA that you’re making, but now you’ve
dysregulated the methylation machinery so you’ve woken up your endogenous virome and then
those RNAs like syncytin are going to be expressed.
Judy Mikovits:
And that’s why we’re seeing older and older women saying, “Oh, there’s menstrual cycles.” And
remember in ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome), you saw the
problems magnified at puberty and menopause. So when those hormones change and you’ve
crippled your liver Kupffer cells or they have to manufacture, they lose latency of the viruses and
just continue to totally disrupt the type I interferon pathway. So it’s actually diabolical and
sinister as we appreciate going back to our friend, Dr. Tony Fauci. What did he do?
Dr. Joseph Mercola:
Your friend.
gammaretroviruses for years. So those people are the ones most likely to sustain the quick injury
because they already have at the heart, all the way back, Dr. Jonathan Kerr, the first things I did
in 2006 is get that type I interferon pathway on and restore DNA methylation. So
dimethylglycine right now as a supplement along with glutathione because you’ve got to keep the
flame turned down so that the pathway doesn’t get further. So everything about this vaccine goes
back. This is why people with HIV-1 infections, this is why people with diseases that look like
that, that inflammatory signature disease, multiple sclerosis; anybody with these genetic
pathways epigenetically dysregulated by the toxins, that’s why aluminum, everything we know in
vaccine injury is translatable to this problem and we can fix it.
Judy Mikovits:
So yes, it’s a problem, but you, Joe, Stephanie, we’ve been addressing this problem for at least in
my life, the last 15 years. So the solutions make sense. They’re the same solutions, ivermectin,
hydroxychloroquine, low-dose antiretroviral therapy, rather natural product or otherwise so we
can educate our immune systems. Type I interferon, peptide Ts, cannabis, all those things we’ve
been talking about for the last three years. We predicted the problem. And now that the problem
is, yes, it’s far worse than we expected, but I don’t see gloom and doom. I see an opportunity, but
we have to make it evident that we appreciate the mechanisms.
Dr. Joseph Mercola:
What I want to understand is a deeper level too because we are giving these messenger RNA
vaccines and in a moment I want you to give your impression of how the Johnson & Johnson
adenovirus vaccine differs from that. But essentially we’re giving this messenger RNA, which is
being converted back to DNA and integrated into the genome. So essentially these people who
are immunized are essentially producing these genetically altered spike proteins on a regular
basis, *in many cases for the rest of their lives. And what you mentioned about the GC-rich
residues activating the latent viruses, when these viruses are activated, do these sequences also
get integrated in our genome?
Judy Mikovits:
They can, but it depends on the defective levels that you need. You need an integrase gene along
the same time. So the answer is yes. And even if a portion gets in, but you won’t integrate in the
genome because the sequences won’t be expressed unless a cell is dividing. So when you’re at
homeostasis in your immune system. So the people at most risk are people with cancer or with
inflammatory diseases because by definition cells are dividing. As Stephanie said in the
beginning when you start to see wounds and skin lesions and things where it’s clear a herpetic
infection is going on, what you have to do is restore the balance to the playing field. Go use a
combination of drugs to enhance methylation like dimethylglycine. That’s not even a drug, that’s
a nutrient. You can use dimethylglycine, betaine.
Dr. Joseph Mercola:
I’m assuming trimethylglycine would work too.
Judy Mikovits:
Both. Yes.
Stephanie Seneff:
That’s betaine. I think that is trimethylglycine, betaine.
Judy Mikovits:
Yeah. Betaine is trimethylglycine.
Stephanie Seneff:
B10 and betaine, oh, that’s good. It’s interesting that it’s glycine too because I have a feeling that
relates to glyphosate.
Judy Mikovits:
Correct, because you’re crippling your [inaudible 00:35:52] so I’ve been encouraging and we’ve
been looking at, keep the playing field level. All of the viruses are activating and this is what
we’ve known. We’ve always seen the bigger problem is the extracellular vesicles packaging all
that RNA because the only time under electron microscopes where you can – and this is always
the argument of Kaufman and others who say, “Oh, it’s just the extracellular vesicles and there
aren’t viruses.” No, the extracellular vesicles are there, but they can package defective viruses.
They can pick up all that RNA because that’s their job.
Judy Mikovits:
The macrophages are going to take that and then drive it into, and then the cells are going to send
the firetruck to the fire. So we never see a disease like let’s just say autism, CFS, AIDS,
everything we saw, under the electron microscope you see 10 times more exosomes in these
patients, even if you don’t find any virus at all. And so the virus in the signaling pathways are
totally dysregulated. So those people have to be protected because they already have membrane
problems, cholesterol diseases. Then you’re going to crank up and further dysregulate ACE2
receptors in those and [inaudible 00:37:24 (angiotensins)]. So I see the problem, almost worse with the
synthetic lipid nanoparticles.
Dr. Joseph Mercola:
Sure. Stephanie, I’ll give you a chance to respond because [crosstalk 00:37:34].
Stephanie Seneff:
Yeah, this is all very fascinating.
Dr. Joseph Mercola:
What’s your take on that?
Stephanie Seneff:
Yeah. I want to say that I told Judy, sometime ago that I was really, really determined to try to
get her stuff and my stuff to merge. And I think we’re a lot closer to that now than we were a
year ago. I hope Judy agrees with that, but I got really hung up on this prion angle towards the
end of our paper. We knew about some hints about a spike protein being a prion. And at the time
we decided maybe it’s too immature, we’ll leave it out of the paper. And then fortunately one of our reviewers said You need to cover this. So we went back to the drawing board to cover it a bit deeper; and I think we dug out a gold mine, it was absolutely terrifying to me and I’m now thinking that may be the worst aspect of these messenger mRNA vaccines because they are producing this abnormal spike protein that doesn’t want to go through the membrane. Prion proteins are known to be typically membrane proteins in the membrane and when they misfold …they’re alpha-helixes in the membrane and then they misfold and become bets sheets in the cytoplasm. That’s what leads to the prion problem they form like a crystal that draws in other proteins and makes like a big mess, and build these fibrils? and what-not, things like Alzheimer’s plaques, … the main prion protein is PRP which is in the Creuzfeld-Jacob’s disease, the human form of mad cow - and we had all that mad cow stuff going on with the cows in the UK, everyone knows about that, it’s kind of a proton (protein?) source infection, it’s quite wild because there’s no DNA involved, no RNA, just protein. But the thing is, when you have produced a version of messenger RNA that knows how to spew out tons of a prion protein, the prion proteins become problematic when there’s too many of them, when the concentration is too high in the cytoplasm, and these spike proteins, that these messenger RNA vaccines are producing, first of all they are producing many because they have manipulated the RNA to make it better able to make protein, and they’re making this version that is not able to go into the membrane, and I think that’s gonna encourage it to be more likely to become a problematic prion protein.
(Continues below)